Category: Stroke | Vascular Dementia | Neurovascular
Clinical Summary
A 76-year-old man was brought to the NeuroMet OPD by his son, himself a known patient at the clinic, with a three-month history of progressive forgetfulness and mild slurring of speech. What appeared on the surface to be age-related cognitive decline turned out to be something far more urgent: an active acute ischemic stroke layered over a background of multiple prior strokes and chronic microvascular disease. This case is a reminder that in neurology, a calm presentation can hide a brewing catastrophe, and that a neurologist's instinct, backed by the right imaging done at the right time, can be life-saving.
Patient Presentation
The patient was a 76-year-old male with a 16-year background of both diabetes mellitus (high blood sugar) and hypertension (high blood pressure), two of the most significant long-term risk factors for stroke and vascular brain disease. He arrived at the clinic accompanied by his son, who was a known patient of mine being treated for a separate neuropathic condition. This family connection meant I had some contextual trust established, but what I observed in the father immediately raised clinical alarm bells.
His primary complaints were two-fold: progressive forgetfulness over the preceding three months, and mild slurring of speech that had also developed during the same period. His family noted that he could recall old memories with reasonable clarity, but new memory formation was significantly impaired ; he would forget recent conversations, lose track of daily tasks, and repeat himself. The speech slurring was mild but consistent, present daily rather than episodic.
There was no reported sudden headache, no loss of consciousness, no visible limb weakness at home, and no prior documented stroke history, though the imaging would later tell a very different story about what had silently occurred inside his brain.
Clinical Examination
On examination at the NeuroMet OPD:
- Blood pressure: 140/90 mmHg, mildly elevated, consistent with his known but incompletely controlled hypertension
- Neurological examination: Cognitive impairment was evident on bedside testing, consistent with short-term memory deficits; speech was mildly dysarthric (slurred but comprehensible)
- Motor examination: Bilateral lower limb weakness was noted on history; detailed motor testing confirmed mild weakness
- Cerebellar examination: No frank ataxia
- Cranial nerves: No additional focal deficits detected
The combination of subacute cognitive decline, vascular risk factor background, bilateral lower limb involvement, and new dysarthria in a 76-year-old diabetic hypertensive patient made this a neurological emergency in my assessment, even without the dramatic presentation of a classic stroke.
Investigations and Findings
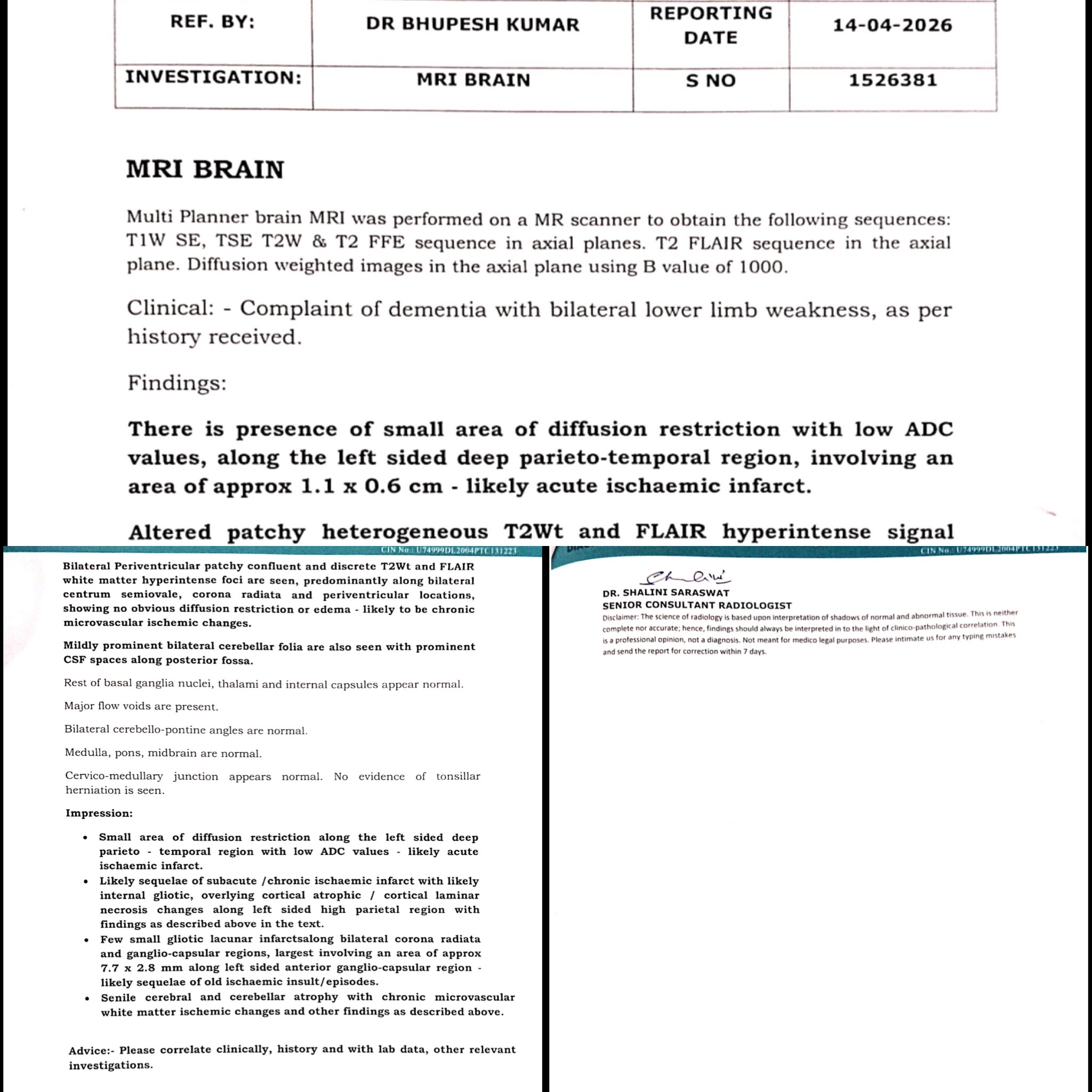
MRI Brain (April 2026)
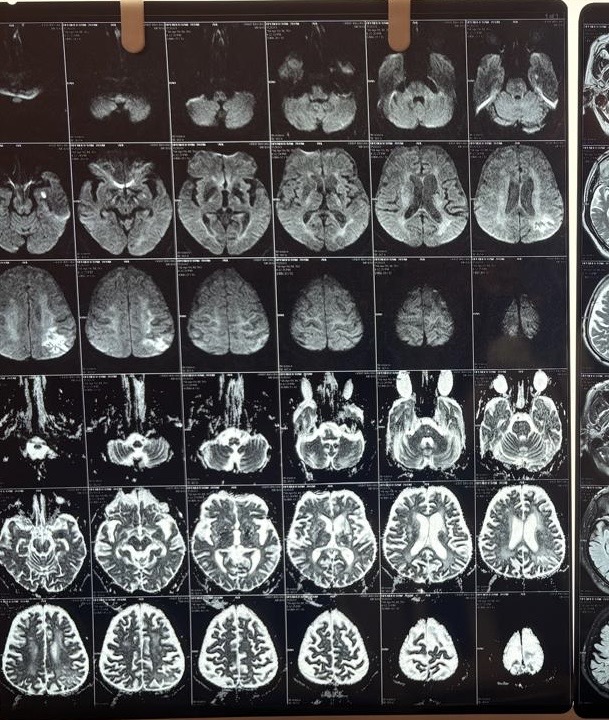
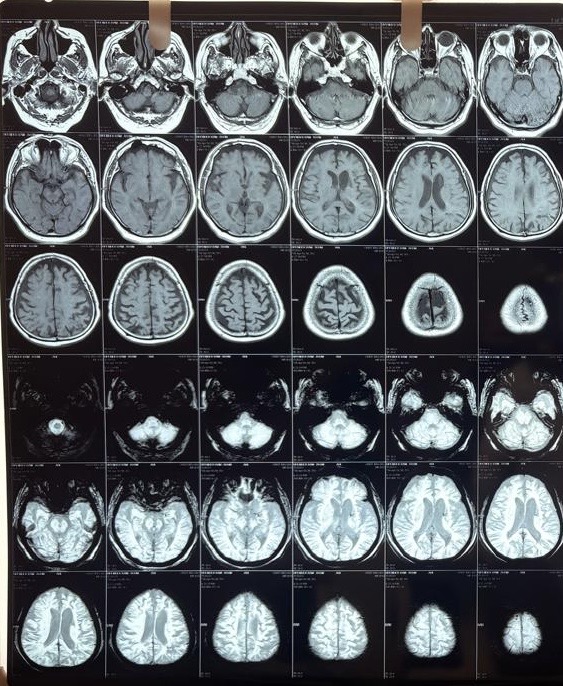
This was the critical investigation. The MRI brain with DWI (diffusion-weighted imaging), FLAIR, and T2 sequences revealed a layered, complex picture:
Acute ischemic infarct:
A small area of diffusion restriction with low ADC values (a pattern on MRI that indicates fresh, actively dying brain tissue) was identified in the left deep parieto-temporal region, measuring approximately 1.1 x 0.6 cm. This confirmed an acute ischemic stroke (a new blockage of blood supply to a specific brain region) was occurring at or around the time of presentation.
Subacute/chronic left parietal infarct:
A larger heterogeneous T2/FLAIR hyperintense lesion in the left high parietal region (approximately 3.1 x 3.3 cm) showed mixed features: internal gliotic areas with CSF FLAIR suppression, irregular peripheral diffusion restriction with high ADC values, overlying cortical atrophic changes, and subcortical gyriform T1 hyperintensities. This pattern was consistent with sequelae of a subacute to chronic prior infarct with cortical laminar necrosis (scarring of the cortical surface following prolonged ischemia))*; indicating a prior stroke that had likely gone undiagnosed.
Old lacunar infarcts:
Multiple small gliotic lacunar infarcts (tiny old stroke scars from small vessel disease) were seen bilaterally in the corona radiata and ganglio-capsular regions, the largest approximately 7.7 x 2.8 mm in the left anterior ganglio-capsular region.
White matter disease:
Bilateral periventricular and centrum semiovale T2/FLAIR hyperintense white matter foci without diffusion restriction, consistent with chronic microvascular ischemic changes (long-standing small vessel damage due to diabetes and hypertension).
Cerebral and cerebellar atrophy:
Diffuse senile atrophy (age-related brain shrinkage) was noted across both cerebral hemispheres, most prominent in the fronto-parietal regions, along with mild cerebellar atrophy. This contributed to the cognitive picture.
The brainstem, basal ganglia, thalami, internal capsules, major intracranial vessels (flow voids), and cerebellopontine angles were all intact.
Blood Investigations (April 2026)
| Parameter | Value | Reference | Significance |
|---|---|---|---|
| Haemoglobin | 12.2 g/dL | 13.5–18 | Mild anaemia, can compound cerebral ischemia |
| RBC Count | 4.62 mill/cu.mm | 4.7–6.0 | Low normal |
| PCV | 39.5% | 42–52% | Low, supports anaemia |
| RDW | 18.7% | 11.5–14 | Elevated, anisocytosis, mixed deficiency likely |
| MCH / MCHC | 26.5 / 30.9 | Low | Hypochromic pattern |
| Platelet count | 169 x 10³/µL | 150–450 | Normal |
| MPV | 11.9 fL | 6–9.5 | Elevated, larger platelets, higher thrombotic risk |
| PDW | 19.4% | 9–17 | Elevated, platelet activation marker |
| Creatinine | 1.24 mg/dL | 0.72–1.25 | Upper normal, monitor drug dosing |
| Potassium | 5.01 mmol/L | 3.5–5.1 | Upper normal, monitor with ACE inhibitors |
| Chloride | 96.90 mmol/L | 98–107 | Mildly low |
| Magnesium | 2.65 mg/dL | 1.8–2.4 | Mildly elevated |
| Vitamin D (25-OH) | 23.60 ng/mL | Sufficiency >30 | Insufficient, relevant in fall risk and immunity |
| CRP | 0.68 mg/L | <6 | Normal, no acute inflammatory/infective trigger |
| ESR | 22 mm/hr | 0–30 | Normal |
The elevated MPV and PDW are particularly noteworthy in a stroke context: they reflect heightened platelet reactivity and are associated with increased ischemic stroke risk and recurrence. The mild anaemia (likely mixed, iron deficiency given the pattern) is clinically relevant as it reduces oxygen delivery to already ischemic brain tissue. CRP and ESR being normal effectively ruled out an infective or inflammatory aetiology.
Glucose Random and Urine RE/ME could not be collected (sample not received) and will need to be recollected.
Diagnosis
Primary Diagnosis:
- Vascular Dementia (F01.50) (memory and cognitive loss caused by accumulated brain damage from multiple strokes and small vessel disease)
Concurrent Active Finding:
- Acute Ischemic Stroke (left deep parieto-temporal region) (small but significant, confirmed on DWI)
Background:
- Subacute/chronic left parietal infarct with cortical laminar necrosis
- Multiple old lacunar infarcts along bilateral corona radiata and ganglio-capsular regions
- Chronic microvascular ischemic white matter disease
- Senile cerebral and cerebellar atrophy
- Mild normochromic-hypochromic anaemia
- Vitamin D insufficiency
- Elevated platelet indices (high MPV, PDW)
The diagnosis of acquired cerebral atrophy was ruled out as the primary diagnosis; the cognitive decline was clearly multifactorial, driven predominantly by cumulative vascular injury rather than pure degenerative atrophy.
Treatment Approach
Given the imaging findings, hospital admission was strongly advised for comprehensive stroke workup, including cardiac monitoring (to rule out atrial fibrillation and cardioembolic source), carotid Doppler, HbA1c, fasting lipid panel, and supervised BP control. The patient and family were counselled at length about the risks of managing an acute stroke in an outpatient setting.
However, due to the absence of health insurance coverage and financial constraints, the family declined admission. A formal informed refusal of admission was documented with consent. Management was then optimized for the outpatient setting.
Medications prescribed:
- Aspirin 150 mg, once daily after dinner: antiplatelet therapy for acute and secondary stroke prevention
- Clopidogrel 75 mg, once daily after dinner, for 21 days only, as dual antiplatelet therapy (DAPT) for the acute stroke window, then to be stopped
- Atorvastatin 40 mg, once daily at night: high-intensity statin (cholesterol-lowering and plaque-stabilizing agent), essential in acute stroke management
- Citicoline 500 mg + Piracetam 400 mg, twice daily: neuroprotective agents (support surviving brain tissue and cognitive function)
- Coenzyme Q10 300 mg, once daily: mitochondrial support and vascular health
- Vinpocetine 10 mg (cerebral blood flow enhancer, once daily)
- Domperidone 30 mg + Esomeprazole 40 mg, once daily on empty stomach: gastric protection with DAPT
Follow-up was scheduled at one month. Pending investigations (glucose random, urine routine examination) were advised to be recollected. BP monitoring at home was advised, with a target below 130/80 mmHg given the stroke and diabetes background. Vitamin D supplementation was also to be addressed.
Outcome and Follow-Up
As of the date of this writing, the patient was discharged on the above outpatient regimen with strict family counselling. The son was advised to monitor for any new neurological symptoms: worsening speech, new limb weakness, loss of balance, sudden confusion, or facial asymmetry, any of which would necessitate immediate emergency hospital presentation. A follow-up appointment is scheduled at one month for repeat cognitive assessment, review of the glucose and urine reports, and consideration of HbA1c, lipid profile, carotid Doppler, and echocardiography.
Clinical Pearls
-
Progressive forgetfulness in a vascular-risk-loaded elderly patient is a stroke until proven otherwise. Do not anchor on "dementia" without imaging. This case had an active acute DWI-positive infarct at the time of OPD presentation.
-
The son's connection made a difference. Established trust with a known family member can lower barriers to early workup. Cognitive decline in an elderly parent brought in by a younger family member warrants a low threshold for urgent MRI.
-
Elevated MPV and PDW are underappreciated stroke biomarkers. In routine CBC in stroke patients, these platelet indices should be flagged; they reflect platelet hyperreactivity and correlate with thrombotic risk, yet are routinely ignored.
-
Acute-on-chronic cerebrovascular disease is common and commonly missed. The radiological layering (acute infarct, subacute infarct with laminar necrosis, old lacunars, and white matter disease) tells the story of years of silent vascular injury finally surfacing as dementia. The acute component in this case was the trigger for immediate antiplatelet and statin therapy.
-
When admission is refused, document meticulously and optimise outpatient management. A signed refusal of admission, thorough family counselling, a clear emergency return plan, and the most evidence-aligned outpatient regimen are non-negotiable medicolegal and ethical steps.
This case was managed by Dr. Bhupesh Kumar Mansukhani, Neurologist and Director, NeuroMet Wellness Care and Diagnostics, Gurgaon. For appointments: www.neurometwellness.com
Disclaimer: Patient details have been de-identified and shared with appropriate consent documentation. This case study is intended for educational purposes only and does not constitute individualised medical advice.
References and Supporting Literature
-
Powers WJ, et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke (2019 Update). Stroke. 2019;50(12):e344–e418. American Heart Association / American Stroke Association. https://doi.org/10.1161/STR.0000000000000211
-
Sachdev P, et al. Diagnostic Criteria for Vascular Cognitive Disorders: A VASCOG Statement. Alzheimers Dement. 2014;10(5):S7–S17. https://doi.org/10.1016/j.jalz.2014.01.007
-
Wardlaw JM, et al. Neuroimaging Standards for Research into Small Vessel Disease. Lancet Neurol. 2013;12(8):822–838. https://doi.org/10.1016/S1474-4422(13)70124-8
-
Bath PM, Krishnan K. Interventions for Deliberately Altering Blood Pressure in Acute Stroke. Cochrane Database Syst Rev. 2014. https://doi.org/10.1002/14651858.CD000039.pub3
-
Katan M, Luft A. Global Burden of Stroke. Semin Neurol. 2018;38(2):208–211. https://doi.org/10.1055/s-0038-1649503
-
Gasparyan AY, et al. Mean Platelet Volume: a Link Between Thrombosis and Inflammation? Curr Pharm Des. 2011;17(1):47–58. https://doi.org/10.2174/138161211795049804