Tags: Vestibular Neuritis | HINTS Exam | Central vs Peripheral Vertigo | PICA Stroke Mimic | Leukodystrophy Mimic | Neurodiagnostics Category: NeuroMet Case Studies
Clinical Summary
A 66-year-old woman was so dizzy she could not get out of bed. Her local doctor had already started treatment for vertigo — but two weeks later, nothing had changed. When she came to the neurology clinic, the first instinct was to rule out a stroke affecting the balance centres of the brain. The MRI brain came back with an alarming-looking report — white matter changes flagged as possible leukodystrophy or metabolic encephalopathy. The cervical spine MRI showed multilevel disc disease and an unexpected soft tissue mass. Yet through it all, the answer lay not in any scan — but in a structured, three-part bedside examination that took less than five minutes to perform. This is a case about the irreplaceable power of clinical neurology, and why a skilled examiner will always outperform an MRI machine when it comes to dizziness.
Patient Presentation
A 66-year-old woman presented to NeuroMet with a 2–3 week history of severe, continuous vertigo (a false sensation of spinning or movement, distinct from general light-headedness) and giddiness that had left her almost entirely bedridden. The onset had been subacute — not a sudden thunderclap, but a rapidly progressive inability to function.
She had already been evaluated by a local general practitioner, who had initiated treatment with Betahistine Dihydrochloride 16 mg twice daily (a vestibular suppressant commonly used for inner ear disorders) and Prochlorperazine 5 mg (an antiemetic and anti-vertigo agent). Despite adequate duration of therapy, there was no meaningful clinical improvement. The severity of her symptoms was such that she was unable to stand or walk independently, prompting referral for specialist neurological evaluation.
There was no history of sleeping in an awkward neck position, no preceding upper respiratory tract infection noted at this stage, no significant ear pain or hearing loss reported, and no prior similar episodes. She had no focal weakness, no diplopia, no dysphagia, and no loss of consciousness.
Clinical Examination & Initial Workup
General and Neurological Examination:
Consciousness was intact, orientation preserved. Limb power and sensory examination were normal bilaterally. No cerebellar signs on finger-nose or heel-shin testing. No focal cranial nerve deficit.
The dominant and disabling symptom was persistent rotatory vertigo with marked nausea, significantly worsening on any head movement.
Given her age, the severity of symptoms, their treatment-refractory nature, and the absence of an obvious peripheral cause, the clinical suspicion was immediately raised for a central cause of vertigo — specifically a PICA territory stroke (infarct in the posterior inferior cerebellar artery territory, a well-recognised cause of acute severe vertigo that can mimic peripheral vestibular disease).
Investigations & Findings
MRI Brain with Contrast (02 Feb 2026 — Krishna Diagnostics)
The MRI brain report described:
- Symmetrical confluent FLAIR hyperintensities (bright signal areas on the MRI) involving the periventricular white matter, corona radiata, centrum semiovale, basal ganglia, internal capsules, cerebral peduncles, and mild involvement of the splenium of corpus callosum — without mass effect or post-contrast enhancement
- A 7.3 × 5.7 mm hypointense lesion in the anterior vermis (a small lesion in the lower part of the cerebellum) — likely calcified, with minimal surrounding oedema and no enhancement
- Mild age-related cerebral atrophy with small vessel ischemic changes
- No acute infarct. No haemorrhage. No enhancing mass lesion.
- Findings reportedly unchanged from a prior MRI brain study
The radiological impression raised differentials of toxic/metabolic encephalopathy, adult-onset leukodystrophy, and demyelination for the white matter changes.
Critical Clinical Correlation:
A comprehensive metabolic, toxic, and inflammatory workup was initiated — including blood biochemistry, CSF analysis, and relevant serological markers. All investigations returned within normal limits. There was no clinical, biochemical, or CSF evidence to support toxic encephalopathy, leukodystrophy, or an active demyelinating process. The white matter signal changes, in the context of her age, vascular risk factors, and stable prior imaging, were most consistent with chronic small vessel ischaemic changes — a common age-related finding. The MRI findings, while visually striking, did not represent a new or active pathological process, and were not the cause of her acute presentation. This is an important reminder that MRI reports require active clinicoradiological correlation — a radiological flag is not a diagnosis.
The cerebellar vermis lesion (likely calcified granuloma) was noted as an incidental finding requiring surveillance, with no clinical correlate.
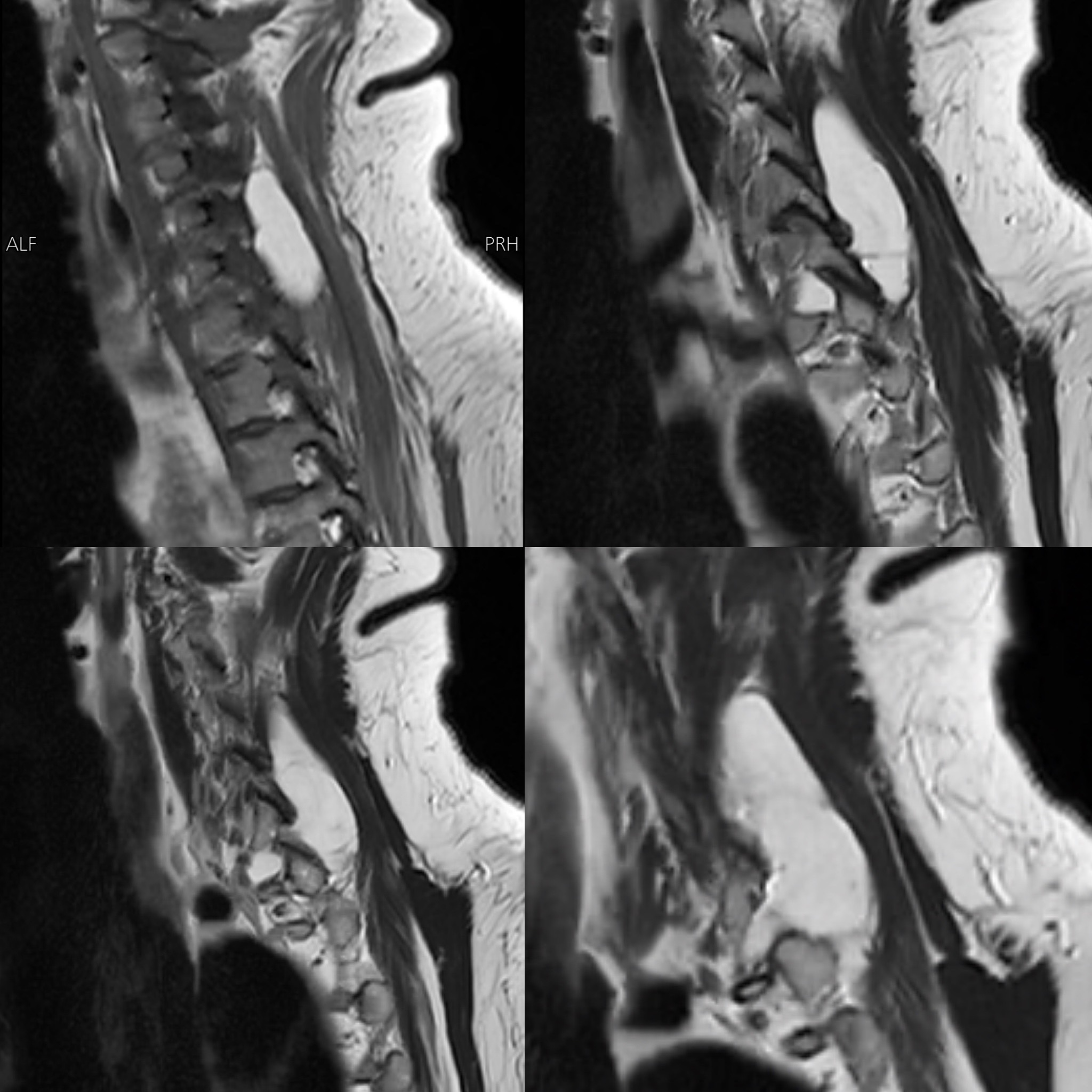
MRI Cervical Spine (31 Jan 2026 — House of Diagnostics, Indirapuram)
- Multilevel cervical spondylosis with disc bulge and annular tears at C4-C5, C5-C6, and C6-C7, causing bilateral foraminal narrowing and mild nerve root impingement (right > left)
- Mild disc changes at C2-C3 and C3-C4 without nerve root impingement
- Straightening of cervical lordosis with mild dextroscoliosis
- Cervical spinal cord: Normal — no signal change, no myelopathy
- A lobulated, well-defined T1/T2 hyperintense lesion in the right posterior paravertebral muscles, extending from C4-C5 to D1 level, measuring 40 × 20 × 54 mm — showing complete fat saturation on STIR sequences, consistent with a benign intramuscular lipoma (a non-cancerous fatty tumour within the muscle), with extension into the right paravertebral gutter and C7-D1 neural foramen causing nerve root compression, but no intraspinal extension and no cord involvement
The cervical spine findings explained her neck pain, but did not account for her acute vertigo presentation. The cord was normal, making cervical myelopathy an unlikely contributor to her primary complaint.
Blood Investigations
Routine haematology, biochemistry, thyroid function, inflammatory markers, and metabolic panel — all within normal limits.
The Diagnostic Pivot — The HINTS Examination
With central pathology excluded on imaging and bloodwork, and with peripheral vestibular suppressants having failed to provide adequate relief, a structured HINTS examination (Head Impulse, Nystagmus, Test of Skew — a validated three-part bedside test to distinguish central from peripheral vestibular disorders) was performed at the bedside.
| HINTS Component | Finding | Interpretation |
|---|---|---|
| H — Head Impulse Test | Positive (corrective saccade seen) | Suggests peripheral vestibular pathology |
| I — Nystagmus | Unidirectional, horizontal, direction-fixed | Consistent with peripheral vestibular disorder |
| T — Test of Skew | Negative (no vertical skew deviation) | No brainstem involvement |
HINTS interpretation: Peripheral pattern — consistent with Vestibular Neuritis.
A positive Head Impulse Test combined with unidirectional, direction-fixed nystagmus and absent skew deviation is the bedside signature of peripheral vestibular pathology. In contrast, a normal or negative Head Impulse Test with direction-changing nystagmus or a positive skew would have strongly indicated a central lesion — and mandated urgent further central workup despite a normal MRI.
The HINTS examination, in experienced hands, has been shown in literature to have sensitivity exceeding 96% for identifying posterior fossa strokes — outperforming even early diffusion MRI, which can miss small posterior fossa infarcts in the first 24–48 hours. In this case, it conclusively supported a peripheral vestibular origin.
Diagnosis
Vestibular Neuritis
(Inflammation of the vestibular nerve — the nerve connecting the inner ear's balance organ to the brain — resulting in acute, severe, prolonged vertigo without hearing loss)
Incidental Findings (not causally related to acute presentation):
- Chronic small vessel ischaemic white matter changes (age-appropriate, stable)
- Benign intramuscular lipoma — right posterior paravertebral region (surveillance recommended)
- Calcified cerebellar vermis lesion — likely granuloma (surveillance recommended)
Treatment Approach
Acute Phase:
- Betahistine Dihydrochloride continued at optimised dosing
- Prochlorperazine continued for nausea and acute vestibular suppression
- Advice on hydration and rest during the acute inflammatory phase
Vestibular Rehabilitation Physiotherapy:
The cornerstone of recovery in vestibular neuritis is not medication — it is structured vestibular rehabilitation. Cawthorne-Cooksey exercises and gaze stabilisation exercises were initiated under physiotherapy guidance. These exercises work by promoting central vestibular compensation (the brain's ability to recalibrate its balance processing when one inner ear is sending abnormal signals) — a process that is actively hindered by prolonged immobility or over-reliance on vestibular suppressants.
Key counselling point: The patient and family were reassured that vestibular neuritis, while severely debilitating acutely, carries an excellent prognosis with structured rehabilitation. The MRI findings were explained in detail — the white matter changes were clarified as chronic, age-related, and clinically non-contributory to her current episode.
Outcome & Follow-Up
With optimised medication and commencement of vestibular physiotherapy, the patient began showing gradual improvement in her ability to mobilise. The bedridden state resolved progressively as vestibular compensation was established. Follow-up was scheduled for neurological reassessment, and the patient was counselled regarding the paravertebral lipoma and cerebellar vermis lesion — both requiring periodic imaging surveillance rather than immediate intervention.
Clinical Pearls / Teaching Points
-
The HINTS exam is a superpower at the bedside. In acute severe vertigo, a structured HINTS examination by a trained neurologist can reliably distinguish central from peripheral vestibular pathology — and in some studies outperforms early MRI-DWI for posterior fossa strokes. Every neurologist should be fluent in performing and interpreting it.
-
An alarming MRI report is not always an alarming disease. Radiological descriptions of white matter changes — even those using words like "leukodystrophy" or "metabolic encephalopathy" — must always be interpreted in full clinical context. When comprehensive blood, CSF, and clinical workup is negative, and findings are stable on serial imaging, these changes are often chronic small vessel disease. Treating the report instead of the patient is a diagnostic trap.
-
Failure to respond to vestibular suppressants should trigger a neurological review — not just dose escalation. This patient had been on Betahistine and Prochlorperazine for weeks without relief. This red flag warranted specialist evaluation and ruled out a central cause before confirming the peripheral diagnosis.
-
Vestibular rehabilitation is the treatment, not an afterthought. Medication manages symptoms acutely; vestibular physiotherapy drives recovery. Early initiation of Cawthorne-Cooksey and gaze stabilisation exercises significantly shortens recovery duration and prevents chronic dizziness.
This case was managed by Dr. Bhupesh Kumar Mansukhani, MBBS (Australia), MD (Medicine), DM (Neurology), Fellow in Stroke Medicine and in Advance Neurological Disorders (Harvard Medical School, USA) — Neurologist & Director, NeuroMet Wellness Care and Diagnostics, Gurgaon. For appointments: www.neurometwellness.com | Personal Website: www.drbhupesh.com
Patient details have been de-identified and shared with appropriate consent. This case study is for educational purposes only.
References
- Kattah JC et al. — HINTS to Diagnose Stroke in the Acute Vestibular Syndrome. Stroke. 2009;40(11):3504–3510.
- Newman-Toker DE et al. — HINTS Outperforms ABCD2 to Screen for Stroke in Acute Continuous Vertigo and Dizziness. Acad Emerg Med. 2013;20(10):986–996.
- Tarnutzer AA et al. — Does my dizzy patient have a stroke? A systematic review of bedside diagnosis in acute vestibular syndrome. CMAJ. 2011;183(9):E571–592.
- Strupp M, Brandt T. — Vestibular Neuritis. Semin Neurol. 2009;29(5):509–519.
- Magnusson M, Karlberg M. — Peripheral vestibular disorders with acute onset of vertigo. Curr Opin Neurol. 2002;15(1):5–10.
- Fazekas F et al. — Pathologic correlates of incidental MRI white matter signal hyperintensities. Neurology. 1993;43(9):1683–1689. (Context for white matter changes in aging)