Clinical Summary
A young girl had never been able to lift her right arm properly, not once in her entire life. By the time she reached our clinic, she was 6 years old, had seen multiple neurologists and physicians, and still had no confirmed diagnosis. Her story is a reminder that neonatal brachial plexus palsy (a nerve injury at birth that affects arm movement) can go undiagnosed for years, and that when the right investigation is finally done, the answer is unmistakable.
Patient Presentation
A 6-year-old girl was brought to NeuroMet Wellness Care and Diagnostics by her father, with a chief complaint of inability to raise her right arm beyond 10 degrees of elevation, a limitation present since birth.
The birth history was telling. She had been delivered via breech presentation (feet-first rather than the normal head-first position), a delivery mode associated with significant mechanical stress on the neck and shoulder region of the newborn. No NICU stay was required after birth, but the family noted right shoulder dysfunction from the very beginning.
At approximately one year of age, she had been evaluated at a tertiary center where nerve conduction studies were performed, with a finding suggestive of right ulnar neuropathy (damage to one of the main nerves of the forearm and hand). She was advised physiotherapy and neurosurgical review at the time. The family did not follow up.
Over the subsequent years, she consulted multiple specialists across different centers. No definitive diagnosis was established. Treatments were initiated on a symptomatic basis without a unifying structural explanation for her deficits. The child grew, adapted, and compensated, but her right arm remained largely non-functional for overhead movement.
When her father described the history in detail at our clinic, the combination of breech delivery, shoulder dysfunction from birth, and the pattern of weakness pointed clearly in one direction.
Clinical Examination
On examination, the child was alert, cooperative, and in no distress. General habitus was lean with notably reduced muscle bulk over the right shoulder girdle.
Neurological examination of the right upper limb revealed:
- Active range of motion severely restricted: right shoulder abduction and forward flexion limited to approximately 10 degrees
- Deltoid and supraspinatus (shoulder-lifting muscles) grossly weak and visibly atrophied
- Biceps and brachioradialis (elbow flexors) also weak
- Wrist and finger movements relatively preserved, consistent with sparing of the lower plexus (C7, C8, T1)
- Sensory examination showed reduced sensation over the right lateral arm and forearm
- No Horner's syndrome (drooping eyelid and pupil changes that would suggest a more severe root-level injury)
- Reflexes: biceps and brachioradialis diminished on the right; triceps intact; all lower limb reflexes normal
The pattern was consistent with an upper trunk brachial plexus lesion (C4, C5, C6 distribution), also known as Erb's palsy (paralysis of the shoulder and upper arm muscles following a specific nerve injury).
Investigations and Findings
Nerve Conduction Studies and EMG
Nerve conduction studies (NCS) and electromyography (EMG) were performed at NeuroMet. Motor NCS of bilateral median and ulnar nerves showed distal latencies, CMAP amplitudes, and conduction velocities all within normal limits. F-wave studies were normal bilaterally. Sensory NCS of bilateral median and ulnar nerves were similarly normal.
Needle EMG was performed bilaterally in the deltoid muscles. Insertional activity was normal, no spontaneous activity was seen, and motor unit action potential morphology and recruitment were within normal parameters.
The EMG sampling was intentionally limited given the child's age, extremely lean body habitus, and the real risk of complications with deep muscle penetration in a pediatric patient with minimal muscle bulk. This was a clinically appropriate decision that prioritized safety over exhaustive sampling.
The electrophysiology results, while reassuring against active axonal degeneration in the sampled muscles, did not exclude a preganglionic injury (damage at the nerve root level, proximal to where electrical testing can reliably detect it). In preganglionic avulsion injuries, the nerve root is torn from the spinal cord itself; the peripheral segment beyond the dorsal root ganglion remains intact and conducts normally on NCS, which is precisely why imaging is indispensable in this setting.
MRI Cervical Spine
MRI of the cervical spine demonstrated:
- Straightening of the normal cervical lordosis (the usual inward curve of the neck was flattened), consistent with longstanding postural adaptation
- No disc herniation or canal stenosis at any level
- Cord signal and diameter normal throughout
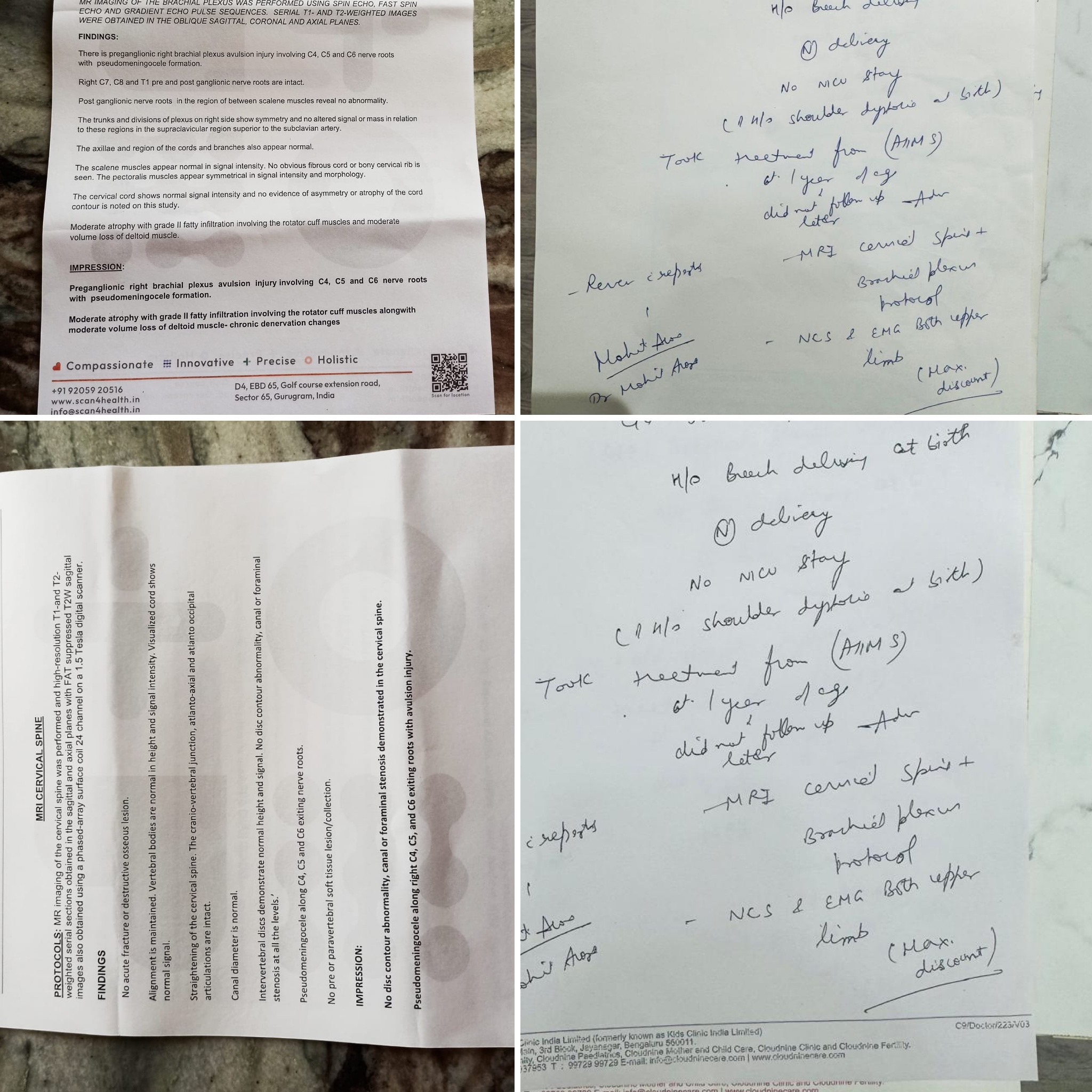
- Pseudomeningoceles at C4, C5, and C6 nerve root exit zones on the right side: outpouchings of the spinal fluid sac that form when nerve roots are torn away from the spinal cord, leaving a gap that fills with fluid. This is a radiological hallmark of preganglionic nerve root avulsion (complete tearing of the nerve from its origin within the spinal cord itself)
MRI Right Brachial Plexus
The dedicated brachial plexus MRI confirmed:
- Preganglionic right brachial plexus avulsion at C4, C5, and C6 with pseudomeningocele formation: the nerve roots were avulsed (torn away completely) from the spinal cord
- C7, C8, and T1 nerve roots intact bilaterally, explaining preserved hand function
- Post-ganglionic nerve roots between the scalene muscles showed no abnormality
- Trunks, divisions, and cords of the right plexus showed normal signal and symmetry in the supraclavicular region
- Moderate atrophy with Grade II fatty infiltration of the right rotator cuff muscles (partial replacement of muscle tissue with fat, indicating longstanding nerve deprivation) and moderate volume loss of the right deltoid, classified as chronic denervation changes
These findings explained everything: this child had never been able to lift her arm because the very nerve roots that power shoulder elevation had been torn from the spinal cord at the moment of her birth.
Diagnosis
Neonatal Brachial Plexus Palsy (Erb's Palsy), Upper Trunk (C4, C5, C6) Preganglionic Avulsion Injury at Birth, with Chronic Denervation Changes
This had been a missed diagnosis for five years. The earlier label of "right ulnar neuropathy" at one year of age was an incomplete characterization that likely reflected a partial electrophysiological finding in a young infant, without the benefit of a dedicated brachial plexus MRI.
The key differentials considered and effectively ruled out included:
- Isolated ulnar neuropathy: excluded by the pattern of weakness (shoulder-dominant, not intrinsic hand muscles) and MRI findings
- Cervical cord pathology: cord signal and contour were entirely normal
- Peripheral nerve tumour or compressive lesion: no mass, no foraminal or canal stenosis identified
Treatment Approach
Given the confirmed preganglionic avulsion at C4, C5, and C6 with significant chronic muscle changes, the management approach was discussed comprehensively with the family.
For preganglionic avulsion injuries of this severity and chronicity, direct nerve repair at the avulsion site is not surgically feasible. The nerve roots are disconnected from the spinal cord itself, not simply torn in the neck where they could be rejoined. The realistic options at this stage include:
- Neurosurgical referral to a dedicated brachial plexus reconstruction unit for evaluation of nerve transfer feasibility (using healthy donor nerves to reroute signals to the paralyzed muscles): a referral was initiated. Orthopedic input may be considered at a later stage for secondary procedures such as tendon transfers or shoulder stabilization, but the primary decision-maker at this point is the neurosurgeon.
- Structured physiotherapy focused on maintaining joint mobility, preventing contractures, and optimizing function of preserved muscle groups
- Occupational therapy for functional adaptation and assistive strategies
- Family counselling regarding realistic expectations given the chronicity and degree of muscle atrophy already established on imaging
Outcome and Follow-Up
The family had clarity for the first time in six years. The diagnosis, though sobering, was definitive, and a structured pathway was now in place. The child was referred for neurosurgical opinion regarding nerve transfer feasibility, and physiotherapy was initiated concurrently. Follow-up was scheduled at NeuroMet to monitor progress and coordinate multidisciplinary input.
Clinical Pearls
-
Breech delivery plus arm weakness from birth should trigger early brachial plexus MRI. NCS/EMG alone are insufficient to characterize preganglionic injuries, where the lesion is proximal to what standard electrophysiology can reliably detect. A normal NCS in this context does not rule out avulsion.
-
Pseudomeningocele on MRI is pathognomonic of nerve root avulsion. Its presence confirms a preganglionic injury and effectively rules out surgically repairable post-ganglionic lesions in that root distribution.
-
In pediatric patients with extremely lean habitus, needle EMG carries real procedural risk. Clinical and imaging judgment must guide how aggressively electrophysiology is pursued. MRI brachial plexus protocol is the non-invasive gold standard for structural characterization in this population.
-
Years of diagnostic delay do not mean the diagnosis is impossible. A thorough history, pattern recognition, and appropriate imaging can reveal the answer even years later. The key is to keep asking the right questions.
This case was managed by Dr. Bhupesh Kumar Mansukhani, Neurologist and Director, NeuroMet Wellness Care and Diagnostics, Gurgaon. For appointments: www.neurometwellness.com
Disclaimer: Patient details have been de-identified and shared with appropriate consent. This case study is for educational purposes only.
References
- Spinner RJ, Shin AY, Bishop AT. Erb's palsy: surgical treatment options. Hand Clinics. 2005;21(1):99-112.
- Pondaag W, Malessy MJA. The evidence for nerve repair in obstetric brachial plexus palsy revisited. BioMed Research International. 2014.
- Somashekar DK, Yang LJ-S, Ibrahim M, Parmar HA. High-resolution MRI evaluation of neonatal brachial plexus palsy: a promising alternative to myelography. Pediatric Radiology. 2014;44(10):1184-1194.
- Chhabra A, et al. MR neurography of brachial plexus: injury characterization and surgical planning. RadioGraphics. 2013;33(4):911-937.
- Smith BW, Daunter AK, Yang LJ-S, Wilson TJ. Management of neonatal brachial plexus palsy: where have we been and where are we now? Pediatric Neurology. 2018;88:13-21.