TITLE: Recurring Hand Numbness That Was Actually a Stroke: A Thalamic Infarct Case
META DESCRIPTION: A 73-year-old man's evening walk ended in a silent thalamic stroke.
See how a neurologist in Gurgaon diagnosed and managed this urgent case.
PRIMARY KEYWORD: thalamic stroke symptoms Gurgaon neurologist
SECONDARY KEYWORDS: transient ischemic attack,
hand numbness stroke, left thalamus infarct, hypercoagulable state, stroke misdiagnosis,
DAPT stroke treatment
SLUG: thalamic-stroke-hand-numbness-misdiagnosed-tia-gurgaon
INTERNAL LINKS TO SUGGEST: Stroke Clinic at NeuroMet,
Understanding TIA vs Stroke, SPG Migraine Case StudyClinical Summary
When a 73-year-old man developed sudden numbness in his right hand during an evening walk, neither he nor his family thought "stroke." His diabetes history pointed them in one direction. The evening heat pointed them in another. Three episodes across four hours, each resolving spontaneously, made the picture look benign. It was anything but. This case is a reminder that strokes can wear the quietest disguises, and that a calm, methodical neurological workup at the right time can prevent a catastrophic outcome.
Patient Presentation
A 73-year-old male with a background of type 2 diabetes mellitus (a condition where the body cannot properly regulate blood sugar, increasing the risk of blood vessel disease) was referred through a family friend, a plastic surgeon, after an alarming evening.
At approximately 5:00 PM, while on his routine evening walk, the patient noticed sudden-onset numbness restricted to his right hand. The sensation resolved completely by the time he reached home, taking no more than a few minutes. The family initially attributed the episode to his diabetes or to the effects of walking in the summer heat, a plausible but ultimately incorrect explanation.
At 8:00 PM, approximately three hours after the first episode, the numbness returned with the same character, the same side, and resolved again within five minutes. The episodic, stereotyped, and self-resolving nature of these attacks raised the clinical suspicion for crescendo TIA (transient ischemic attack: a brief, warning stroke that resolves completely but strongly predicts an imminent full stroke).
At 9:00 PM, a third episode occurred, this time significantly more intense. At this point, the family contacted their physician friend, who immediately reached out to me. By 10:00 PM when I received the call, the symptoms had resolved once again. Despite the apparent resolution, the pattern was unmistakably worrying. Three stereotyped episodes of unilateral hand numbness within four hours, in a diabetic elderly male, constituted a neurological emergency.
The decision was made to pursue urgent evaluation the next morning at the NeuroMet clinic with an MRI Brain, given that emergency room transfer was not feasible that night due to logistical constraints related to CGHS/ECHS empanelment and insurance. This was a calculated clinical decision: the patient had no ongoing deficits, no speech disturbance, no facial involvement, and no limb weakness at that moment. Families were counseled on red-flag warning signs and instructed to go directly to the nearest emergency department if any new symptom appeared overnight.
Clinical Examination
On presentation at clinic the following morning:
Vitals: Blood pressure 170/93 mmHg, elevated (this is significantly above the normal range of 120/80 mmHg, and in the context of an acute stroke, hypertension is both a risk factor and a reactive response of the brain trying to maintain blood flow to the damaged area). Heart rate 78 per minute, SpO2 98% on room air. It is worth noting that the referring history described the patient as normotensive; the elevated BP recorded at clinic likely represents reactive hypertension (a temporary spike in blood pressure that commonly occurs after a stroke or TIA as the body compensates for reduced cerebral perfusion) and reinforced the urgency of hospital admission.
General Appearance: Alert, oriented to time, place, and person. No distress.
Neurological Examination:
- Higher mental functions: intact
- Cranial nerves: no facial asymmetry, palatal movements normal, no diplopia
- Motor system: power 5/5 in all four limbs, tone normal
- Sensory system: at the time of examination, no active sensory deficit; however, the patient described a lingering mild awareness of the right hand
- Coordination: finger-nose test normal, no dysdiadochokinesia
- Reflexes: symmetric, plantar responses flexor bilaterally
- Gait: normal
The examination was essentially non-focal at the time of clinic presentation, which is typical of completed TIA events. The absence of neurological deficit does not exclude a structural brain lesion, and imaging was urgently proceeded with.
Investigations and Findings
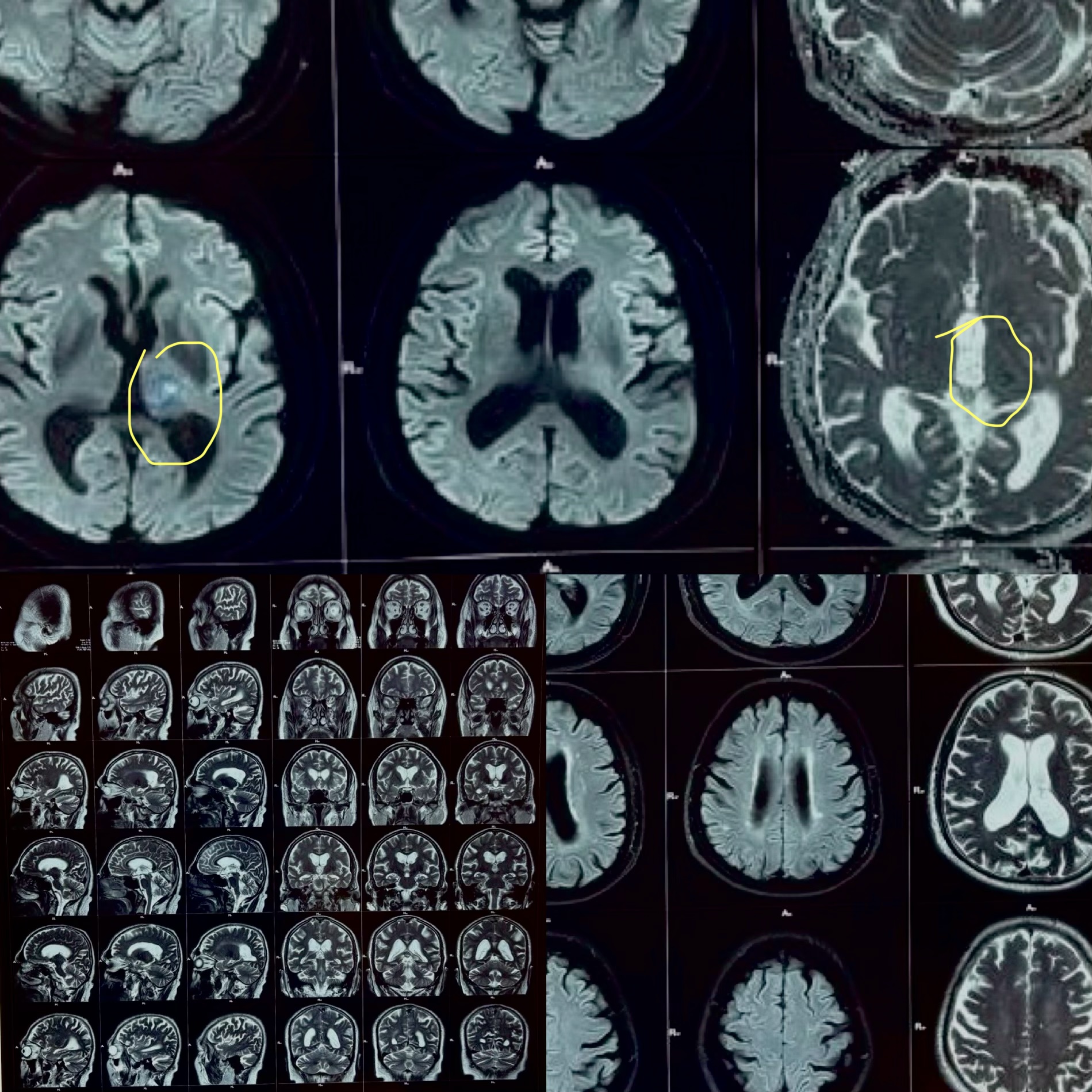
MRI Brain (Mahajan Imaging and Labs, 21 April 2026)
Key Finding: A small, focal area of restricted diffusion in the left thalamus, consistent with an acute ischemic infarct (a tiny area of brain tissue that lost its blood supply and sustained injury, located in the thalamus, the brain's central relay station for sensation and consciousness).
No hemorrhage was identified. No large vessel territory infarction. No mass effect. Ventricular system and basal cisterns appeared normal.
This was the defining finding: the hand numbness was not diabetes-related, not heat-related. It was a thalamic stroke presenting as episodic sensory TIAs before a small completed infarct declared itself.
CTA Brain and Neck (Narula Diagnostics, 22 April 2026)
- No large vessel occlusion (LVO) in the anterior or intracranial circulation
- Bilateral MCA (M1, M2, M3 segments): normal caliber and opacification
- Diffuse atherosclerotic changes (cholesterol and calcium deposits narrowing the arteries) involving the aortic arch, bilateral carotid systems, and cavernous segment of the right ICA (approximately 20-30% stenosis, non-hemodynamically significant)
- Left vertebral artery: diffusely attenuated with distal non-opacification at the intracranial segment, likely representing chronic hypoplasia or old occlusion; posterior circulation maintained via the contralateral right vertebral artery
The CTA offered critical reassurance: no acute large vessel occlusion requiring intervention. The mechanism was likely small vessel or cardioembolic disease in the setting of a hypercoagulable state, atherosclerosis, and poorly controlled diabetes.
Blood Investigations (Medsovis Health Labs, 21-22 April 2026 / Dr. Lal PathLabs, 22 April 2026)
| Investigation | Result | Reference | Comment |
|---|---|---|---|
| HbA1c | 7.8% | Less than 5.7% (non-diabetic) | Suboptimally controlled diabetes |
| Fasting Average Blood Sugar (est.) | 177.41 mg/dL | Less than 135 mg/dL | Elevated |
| Protein S (Free Antigen) | 68% | 70-148% | LOW: suggests hypercoagulable state |
| Protein C (Functional) | 111% | 70-140% | Normal |
| Vitamin B12 | 197 pg/mL | 192-827 pg/mL | Low-normal; borderline |
| Vitamin D3 | 27.3 ng/dL | 30-100 ng/dL (sufficient) | Insufficient |
| Triglycerides | 184.4 mg/dL | Less than 160 mg/dL | Mildly elevated |
| VLDL | 36.88 mg/dL | Less than 30 mg/dL | Elevated |
| LDL | 86.42 mg/dL | Less than 100 mg/dL | Within target for high-risk patient |
| Total Cholesterol | 167 mg/dL | Less than 200 mg/dL | Normal |
| Haemoglobin | 12.4 g/dL | 13-17 g/dL | Mildly low |
| TSH | 3.58 µIU/ml | 0.3-4.5 µIU/ml | Normal |
| CRP (Quantitative) | 1.1 mg/L | Less than 5 mg/L | Normal (no active inflammation) |
| INR | 1.28 | Less than 1.4 | Normal coagulation |
| Renal and Liver functions | Within normal limits | No organ compromise |
The most clinically significant abnormality: Free Protein S at 68%, just below the lower limit of normal (70%). Protein S deficiency (a condition where the blood lacks sufficient levels of a natural blood-thinning protein, making clots more likely to form) is a recognized acquired or hereditary cause of hypercoagulable state (increased tendency of the blood to form abnormal clots). In the context of a thalamic infarct, diffuse atherosclerosis, and suboptimal glycaemic control, this was a significant compounding risk factor.
A 2D Echocardiogram was also performed as part of the stroke workup to rule out a cardiac source of emboli. Results were reviewed in the context of clinical decision-making. No significant structural cardiac abnormality or intracardiac thrombus was identified (details per cardiology review at the admitting hospital).
Diagnosis
Primary Diagnosis: Acute ischemic stroke, left thalamus (small vessel / perforator territory infarct), presenting initially as crescendo TIA (three episodic events over four hours).
Contributing Risk Factors:
- Type 2 diabetes mellitus with suboptimal glycaemic control (HbA1c 7.8%)
- Diffuse atherosclerotic disease (aortic arch, bilateral carotid systems, right ICA cavernous segment)
- Acquired Protein S deficiency (68%): hypercoagulable state
- Left vertebral artery hypoplasia / chronic occlusion (incidental but relevant to posterior circulation reserve)
- Borderline low vitamin B12, insufficient vitamin D
Differentials considered and excluded:
- Diabetic peripheral neuropathy presenting as episodic hand numbness: excluded by MRI evidence of acute infarct and by the stereotyped, episodic, and vascular nature of the attacks
- Cervical spondylosis with radiculopathy: excluded by absence of neck pain, dermatomal pattern, and the ipsilateral thalamic infarct on MRI
- Carpal tunnel syndrome: excluded by bilaterality requirement for that diagnosis not being met and acute onset
- Heat-related autonomic symptoms: excluded by imaging
Treatment Approach
Given the clinical timeline: by the time the patient was assessed and admitted, the thrombolysis window (4.5 hours from symptom onset) had passed. Importantly, the patient had no major neurological deficit at the time of admission, which is consistent with the small size of the infarct and the self-resolving episodic presentation.
Management was guided by American Stroke Association (ASA) 2023-2024 guidelines for minor ischemic stroke and high-risk TIA, specifically the POINT and CHANCE trial data supporting short-term dual antiplatelet therapy.
Treatment regimen initiated:
-
DAPT (Dual Antiplatelet Therapy): Aspirin 150 mg (Ecosprin) + Clopidogrel 75 mg (Plavix). This combination was chosen to prevent early recurrent stroke, supported by robust evidence in minor stroke and TIA patients.
-
High-intensity statin: Rosuvastatin 40 mg nightly. Target LDL less than 70 mg/dL for stroke secondary prevention in high-risk atherosclerotic disease.
-
Citicoline+piracetam: A neuroprotective agent supporting neuronal membrane integrity, commonly used adjunctively in the acute post-stroke period.
-
S-Adenosyl-L-Methionine: To support cerebral blood flow and neuronal metabolism in the peri-infarct region.
-
Multivitamin and antioxidant support, Coq10 300mg: To address the nutritional deficiencies identified (B12 borderline, Vitamin D insufficient) and support vascular health.
-
Gabapentin 100 mg TDS: Initiated for the post-stroke sensory disturbance (thalamic sensory dysesthesia), which can present as uncomfortable tingling or burning sensations in the affected hand following a thalamic infarct.
-
Diabetes optimization: Referred back to the treating physician for adjustment of anti-diabetic medications targeting HbA1c below 7%.
-
Protein S management: Given that acute illness itself can transiently lower Protein S levels, the decision was made to recheck Protein S at 6-8 weeks (off anticoagulation, in a stable state) before labeling it a hereditary deficiency and committing to long-term anticoagulation.
The patient was admitted for 3 days of monitoring, neurological observation, and stabilization of the above regimen.
Outcome and Follow-Up
The patient was discharged on day 3 of admission in a clinically stable condition. No new neurological deficits developed during the admission. The right-hand sensory symptoms had significantly diminished. The patient and family were reassured with a comprehensive discharge plan and a clear understanding of:
- Red flag symptoms requiring immediate ER visit (sudden weakness, speech difficulty, facial drooping, severe headache)
- Medication adherence and the importance of not stopping antiplatelet therapy without medical advice
- Tight glycaemic control as a primary modifiable risk factor
- Repeat Protein S testing in 6-8 weeks
- Follow-up at NeuroMet in 4 weeks
The family expressed complete satisfaction with the clarity of communication, the thoroughness of the workup, and the outcome. The patient left in good spirits, understanding what had happened to him and what was being done to prevent it from happening again.
Clinical Pearls and Teaching Points
For Clinicians
1. Crescendo TIA is a neurological emergency, even when each episode fully resolves.
Three stereotyped episodes of unilateral sensory symptoms over four hours in an elderly diabetic male carries a high early stroke risk. The ABCD2 score and POINT/CHANCE trial data confirm that high-risk TIA patients have a 10-20% risk of stroke within 90 days, with the highest risk in the first 48 hours. Expedited workup is non-negotiable.
2. The thalamus is a great sensory mimic.
Thalamic infarcts in the ventral posterolateral (VPL) nucleus territory present with isolated contralateral hemisensory loss, often mistaken for peripheral neuropathy, carpal tunnel, or radiculopathy. The absence of motor deficits, cranial nerve involvement, or cerebellar signs does not exclude a central lesion. Always image.
3. Protein S deficiency as an acquired stroke risk factor in the elderly.
While hereditary Protein S deficiency is most relevant in young stroke patients, acquired deficiency can occur with acute illness, inflammation, vitamin K deficiency, and liver disease. A value of 68% (below the lower normal of 70%) in the acute setting warrants repeat testing at 6-8 weeks in a stable state before committing to lifelong anticoagulation. Per current ESO (European Stroke Organisation) thrombophilia screening guidance, routine testing is indicated in cryptogenic stroke in younger patients, but clinically relevant borderline values in older patients still merit systematic follow-up.
4. Left vertebral artery hypoplasia and posterior circulation reserve.
The finding of left VA hypoplasia with distal non-opacification is often chronic and incidental. However, it reduces the collateral reserve of the posterior circulation. In the context of a posterior territory infarct (thalamic), documenting this anatomy is important for risk stratification and long-term management discussions.
5. HbA1c at 7.8% in a known diabetic on medications: the glycaemic gap.
Despite being on anti-diabetic medications, this patient's HbA1c remained above the 7% target, signaling suboptimal control over the preceding 8-12 weeks. Diabetes independently accelerates cerebral small vessel disease and endothelial dysfunction. Correcting this gap is as important as the antiplatelet prescription.
For Patients and Families
1. Never wait for the second or third episode.
If a family member develops sudden numbness or weakness, even if it lasts only a few minutes and goes away completely, please do not wait to see if it happens again. That "mini-episode" may be your body's warning siren before a larger stroke. Call a neurologist or go to an emergency room immediately.
2. Diabetes affects your brain, not just your sugar levels.
Poorly controlled blood sugar damages blood vessels throughout the body, including in the brain. Keeping your HbA1c below 7% is one of the most powerful things you can do to protect yourself from stroke. This is not just a number. It is brain insurance.
3. When symptoms disappear, the emergency does not.
The most dangerous misunderstanding in TIA is the belief that "it went away, so we are fine." A TIA is the brain's SOS signal. The window immediately after a TIA is when the risk of a full stroke is highest. Early evaluation and treatment dramatically reduce that risk.
This case was managed by Dr. Bhupesh Kumar Mansukhani, MBBS (Australia), MD (Medicine), DM (Neurology), Fellow in Stroke Medicine and Advanced Neurological Disorders (Harvard Medical School), Neurologist and Director, NeuroMet Wellness Care and Diagnostics, Gurgaon. For appointments and consultations, visit neurometwellness.com/booking.php
Disclaimer: Patient details have been de-identified and shared with appropriate consent. This case study is for educational purposes only and does not constitute medical advice.
References
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
- Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack (CHANCE). N Engl J Med. 2013;369:11-19.
- Johnston SC, Easton JD, Farrant M, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA (POINT). N Engl J Med. 2018;379:215-225.
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update. Stroke. 2019;50(12):e344-e418.
- Arauz A, Murillo L, Marquez JM, et al. Prospective study of single and multiple lacunar infarcts using magnetic resonance imaging: risk factors, recurrence, and outcome in 175 consecutive cases. Stroke. 2003;34(9):2453-2458.
- Pezzini A, Del Zotto E, Magoni M, et al. Inherited thrombophilic disorders in young adults with ischemic stroke and patent foramen ovale. Stroke. 2003;34(1):28-33.
- Ntaios G, Papavasileiou V, Makaritsis K, et al. Hyperglycemia in acute stroke: an update. Eur J Intern Med. 2014;25(4):314-319.