
META DESCRIPTION: A 51-year-old man with disabling
hand tremors was cured not by tremor drugs but by optimizing blood pressure.
Here is what made the difference.
PRIMARY KEYWORD: hand tremor treatment Gurgaon neurologist
SECONDARY KEYWORDS: postural tremor hypertension,
hand shaking high BP, essential tremor vs hypertensive tremor,
tremor neurologist Gurgaon, non-essential tremor diagnosis
SLUG: postural-hand-tremor-hypertension-gurgaon-neurologist
INTERNAL LINKS TO SUGGEST: Cervical Spondylosis and Nerve Compression Cases,
Movement Disorders Clinic, Hypertension and Neurological ComplicationsClinical Summary
Hand tremors are among the most anxiety-provoking symptoms a patient can experience. They disrupt daily tasks, affect confidence, and often prompt a fear of serious neurological disease. Yet in some patients, the tremor is not the primary disease; it is a signal pointing to something else entirely. This case of a 51-year-old man with persistent postural hand tremors illustrates how meticulous clinical reasoning and systematic investigation can uncover a treatable root cause, yielding a complete resolution of symptoms without anti-tremor medication.
Patient Presentation
A 51-year-old gentleman, a known hypertensive, presented to NeuroMet Wellness Care and Diagnostics, Gurgaon, with a chief complaint of persistent shaking of both hands, more noticeable during activity and while maintaining a held position (such as holding a cup or writing). The tremors had been present for several months and were associated with significant anxiety and stress, which the patient himself acknowledged had worsened over the preceding weeks.
He had been on antihypertensive medication for his elevated blood pressure for some time prior to this visit, a combination of spironolactone 25 mg (a diuretic and aldosterone-blocker commonly used for blood pressure and fluid retention) and a fixed-dose combination of telmisartan with hydrochlorothiazide (a pill that blocks a blood pressure hormone pathway while also removing excess fluid from the body via the kidneys). Despite this regimen, his blood pressure remained poorly controlled at the time of evaluation.
His past history was otherwise unremarkable. There was no family history of tremor or movement disorders. He did not consume alcohol and was not on any medication known to cause tremors. He denied any rigidity, slowness of movement, difficulty swallowing, or change in handwriting size, making a Parkinsonian aetiology unlikely from the outset.
Clinical Examination
On examination, the patient was alert and well-oriented. Blood pressure measured at clinic was significantly elevated, consistent with inadequate antihypertensive control. Pulse was regular.
Neurological examination (a structured assessment of the brain, spinal cord, and nerves) revealed the following:
- Postural tremor (shaking that appears when the arms are held up against gravity, as when writing or holding a cup) noted bilaterally in the upper limbs, more prominent on the right.
- Action tremor (tremor that appears during purposeful movement) was also present.
- No resting tremor was identified (which would be a hallmark of Parkinson's disease).
- Tone, power, coordination, and deep tendon reflexes were all within normal limits.
- No bradykinesia (slowness of voluntary movement, a cardinal Parkinson's feature) was detected.
- No cerebellar signs (no dysdiadochokinesia, no gait ataxia).
- Cranial nerves were intact bilaterally.
Systemic examination including cardiovascular auscultation and abdominal examination was grossly normal. A prior 2D echocardiogram (ultrasound of the heart to assess structure and function) had been reported as normal, ruling out cardiac sources of haemodynamic instability.
Investigations and Findings
A comprehensive workup was undertaken to exclude treatable and serious secondary causes of tremor.
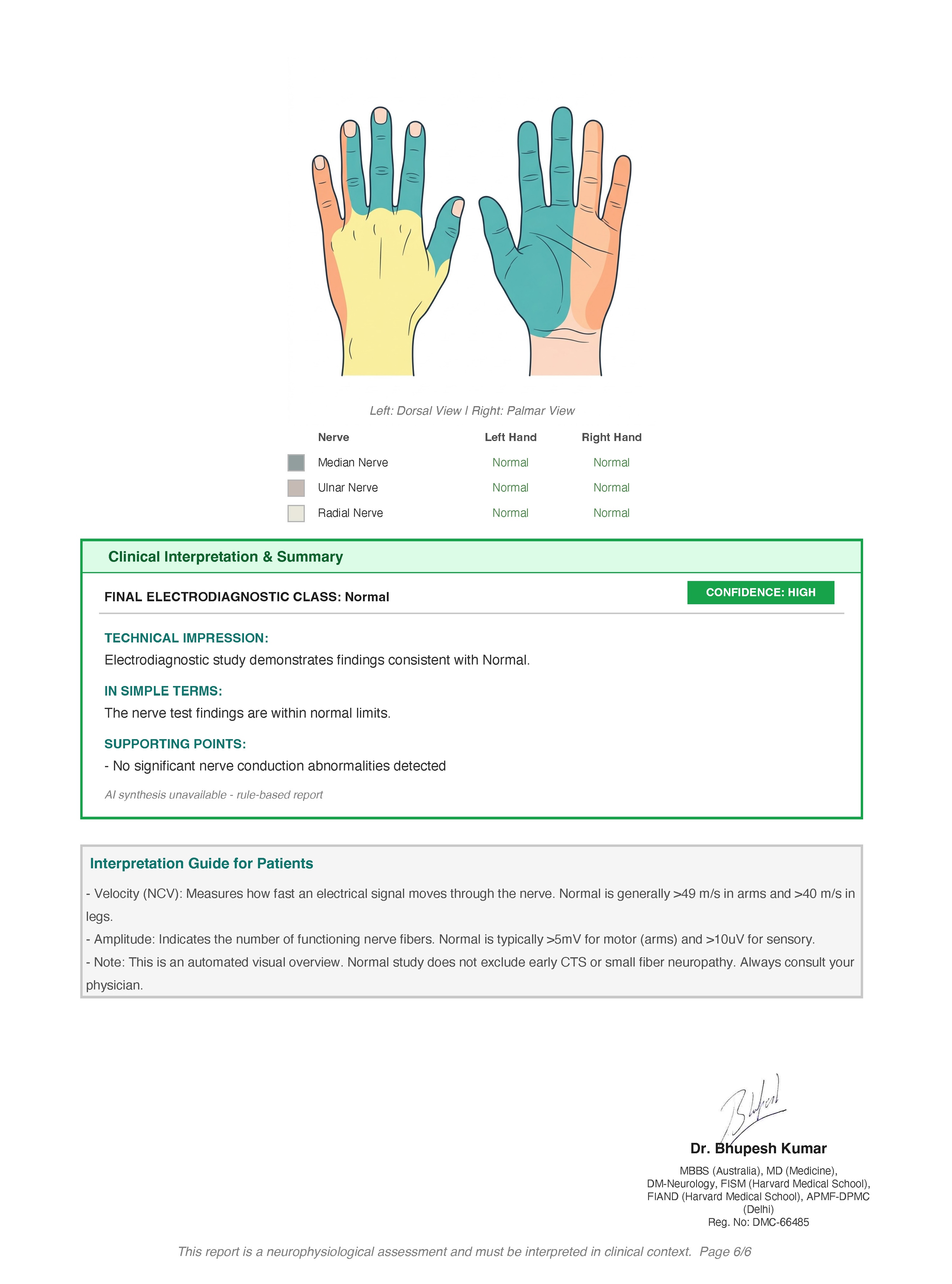
Neurophysiology: NCV and EMG
Nerve conduction velocity (NCV) study (a test that measures how fast electrical signals travel through nerves) and electromyography (EMG) (a test that records the electrical activity of muscles to detect nerve or muscle disease) were performed bilaterally across the median and ulnar nerves of the upper limbs.
- Motor and sensory conduction velocities were normal in all tested nerves.
- CMAP and SNAP amplitudes were within reference range.
- F-wave latencies were normal bilaterally.
- Needle EMG of bilateral flexor pollicis brevis and right biceps brachii showed normal insertional activity, no spontaneous potentials, and normal motor unit action potential morphology with full recruitment.
Conclusion: This study was essentially normal, effectively ruling out peripheral neuropathy, entrapment neuropathy, and neuromuscular junction disease as contributors to the tremor.
MRI Brain
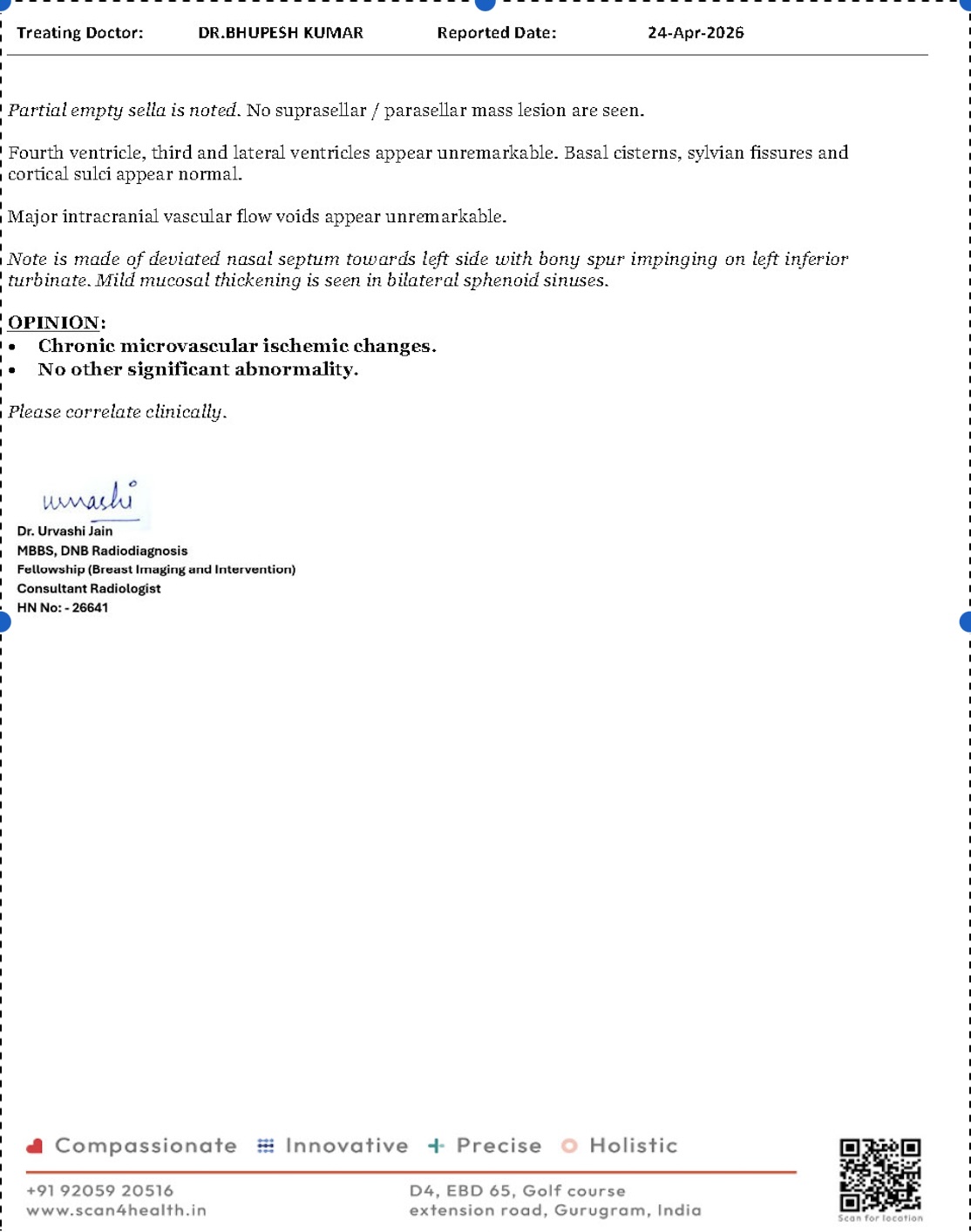
MRI of the brain performed on a 1.5 Tesla digital scanner showed:
- A few focal FLAIR/T2 hyperintensities (small bright spots on a specific type of brain scan) in the supratentorial white matter, without diffusion restriction, consistent with early chronic microvascular ischemic changes (tiny areas of old, non-acute blood vessel-related changes in the white matter of the brain, very commonly seen in people with longstanding hypertension).
- No acute infarct. No space-occupying lesion. No evidence of demyelination.
- Basal ganglia, thalami, cerebellum, and brainstem all appeared normal.
- Pituitary region showed a partial empty sella (a benign finding where the pituitary gland appears partially flattened, of no clinical significance in this context).
This MRI finding was important: it confirmed that hypertension had already begun to leave its fingerprint on the brain's white matter. It also reassured against any structural cause of tremor such as a tumour, stroke, or demyelinating lesion.
MRI Cervical Spine
MRI of the cervical spine revealed multilevel cervical spondylosis (age-related wear and degenerative changes in the bones and discs of the neck), most prominently:
- C4-C5: Posterior disc osteophyte complex with bilateral neural foraminal narrowing and compression of bilateral exiting nerve roots. Canal diameter approximately 11.9 mm.
- C5-C6: Posterior disc osteophyte complex, right greater than left, with bilateral neural foraminal narrowing and exiting root compression. Canal diameter approximately 10.8 mm.
- Cervical spinal cord signal was entirely normal.
While the radiological findings were significant, the normal NCV/EMG conclusively established that these spondylotic changes were not functionally compromising nerve conduction in the upper limbs, making them an incidental structural finding rather than the cause of the tremors.
Blood Investigations
A comprehensive panel was reviewed:
- Haemoglobin: 10.8 g/dL (low), with a pattern consistent with iron deficiency: serum iron 34.6 mcg/dL (low), TIBC elevated at 501 mcg/dL, transferrin saturation reduced to 7%. This would be addressed in the management plan.
- TSH: 10.34 mIU/mL (elevated), with FT3 and FT4 within normal limits, suggesting subclinical to overt hypothyroidism (underactive thyroid gland; an elevated TSH can itself contribute to tremor, fatigue, and exacerbation of cardiovascular risk).
- Autoimmune screen (ANA by IFA, ANCA, RA factor, antiphospholipid antibody panel including anticardiolipin IgG/IgM and anti-beta2-glycoprotein-1 IgG/IgM, lupus anticoagulant): Entirely negative, effectively ruling out autoimmune or inflammatory causes of tremor or neurological involvement.
- CRP: 4.7 mg/L (normal). ESR: 23 mm/hr (mildly elevated, non-specific). No evidence of active systemic inflammation.
- HbA1c: 4.9% (non-diabetic). Fasting lipids: Total cholesterol 216 mg/dL (borderline high), LDL 149 mg/dL (borderline elevated), suggesting cardiovascular risk optimisation is warranted.
- Vitamin D: 51.84 ng/mL (sufficient). Vitamin B12: 248.4 pg/mL (low-normal; monitoring advised).
- Renal and liver function tests: Normal. Electrolytes: Normal.
Diagnosis
After careful clinical assessment and a comprehensive investigation battery, the following conclusions were reached:
Primary diagnosis: Postural hand tremor secondary to poorly controlled hypertension, compounded by anxiety and sympathetic nervous system overactivity.
Supporting diagnosis: Subclinical/overt hypothyroidism (requiring thyroid-directed management). Iron deficiency anaemia. Incidental multilevel cervical spondylosis (radiologically significant, neurophysiologically quiescent).
Differentials considered and excluded: Essential tremor (no family history, atypical pattern, blood pressure clearly uncontrolled), Parkinson's disease (no resting tremor, no bradykinesia, no rigidity), drug-induced tremor (no offending agent identified), Wilson's disease (excluded by clinical profile and age-appropriate presentation), cerebellar tremor (no cerebellar signs clinically or on MRI), peripheral neuropathy (normal NCV/EMG).
The association between postural tremor and incident hypertension has been well established in epidemiological literature, notably the Bogalusa Heart Study, which demonstrated that postural hand tremor is a significant predictor of the development of hypertension in young to middle-aged adults, and conversely, that inadequately controlled sympathetic tone in hypertension can generate or amplify tremor via adrenergic overactivity.
Treatment Approach
The treatment strategy was built around blood pressure optimisation as the primary intervention, with ancillary support for anxiety.
Step 1: Antihypertensive regimen change. The prior regimen was replaced with a single once-daily fixed-dose combination tablet containing telmisartan, amlodipine, and chlorthalidone (a triple-action pill combining a hormone blocker, a calcium channel blocker, and a diuretic for comprehensive blood pressure control with simplified dosing). This was chosen for its superior 24-hour blood pressure control, its favourable metabolic profile, and its potential to reduce adrenergic tremor amplification by achieving steadier, lower blood pressure without reflex sympathetic surges.
Step 2: Anxiolytic support. A low-dose tablet of clonazepam (a medication that calms overactive nerve signals, used here at a very low dose to address anxiety and reduce the neurological sensitisation contributing to the tremor) was introduced once daily at bedtime. This was intended as a short-term adjunct to address the anxiety-stress cycle that was worsening the patient's perception and severity of tremor.
Step 3: Thyroid and haematological workup initiated. Given the elevated TSH and iron deficiency findings, appropriate endocrine consultation and iron supplementation were recommended.
Outcome and Follow-Up
At a review 15 days following the initiation of the revised treatment plan, the patient reported complete resolution of his hand tremors. Blood pressure had come down to target range. His anxiety had significantly reduced. He reported no side effects from the new medications.
The follow-up plan included thyroid function recheck after 6 to 8 weeks, repeat iron studies after a 3-month course of supplementation, and a lipid review for consideration of further cardiovascular risk reduction strategies. Repeat blood pressure monitoring at one month was also scheduled.
Clinical Pearls and Teaching Points
Part A: For Clinicians
-
Hypertension as a tremor amplifier, not just a cardiovascular risk factor. The Bogalusa Heart Study established a bidirectional relationship between postural tremor and hypertension. Adrenergic overdrive in inadequately controlled hypertension lowers the tremor threshold via beta-adrenergic receptor stimulation in skeletal muscle spindles. A trial of improved BP control before escalating to tremor-specific pharmacotherapy is evidence-informed and should be standard practice in hypertensive patients presenting with postural tremor.
-
The normal NCV/EMG is a powerful negative result. In a patient with multilevel cervical spondylosis and hand tremors, there is a very real temptation to attribute the tremor to cervical radiculopathy. Normal nerve conduction and EMG effectively decouple structural cervical disease from functional upper limb involvement. Never treat the MRI; treat the patient.
-
White matter hyperintensities on brain MRI are a radiological biomarker of hypertensive burden. Even in a patient without prior stroke, the presence of confluent or multiple periventricular or subcortical FLAIR hyperintensities should heighten urgency around blood pressure control. Per Fazekas criteria, these findings, while not acutely dangerous, carry long-term risks of cognitive decline and lacunar stroke if the underlying vascular risk is not addressed.
-
Subclinical hypothyroidism elevates tremor risk. A TSH of 10.34 mIU/mL in this patient is significant. Even subclinical hypothyroidism can increase muscle sensitivity to adrenergic stimulation and worsen tremor, fatigue, and cardiovascular risk. The Endocrine Society guidelines recommend treatment when TSH exceeds 10 mIU/mL in symptomatic patients. This finding needed to be addressed as an independent contributor.
-
Anti-tremor drugs should not be the first reflex in hypertensive tremor. Propranolol and primidone, the standard pharmacological tools for essential tremor, carry their own risks in an inadequately worked-up patient: bradycardia, fatigue, potential masking of metabolic disturbances. A structured diagnostic exclusion of secondary causes before initiating tremor-specific agents prevents polypharmacy and unnecessary long-term medication burden.
Part B: For Patients and Families
-
Not all tremors mean Parkinson's disease. This is the fear that most patients carry into the consultation room. Parkinson's disease has a very specific pattern: tremor at rest (when the hand is lying still), combined with slowness of movement and stiffness. Tremors that appear mainly while holding a position or during activity often have other, more treatable causes. Please share your complete history, including all medications and your blood pressure readings, before any diagnosis is assumed.
-
Uncontrolled blood pressure is a brain issue, not just a heart issue. The small bright spots seen on this patient's brain MRI are the result of years of high blood pressure silently affecting tiny blood vessels in the brain. Taking blood pressure medications regularly and monitoring your pressure at home can prevent these changes from progressing to something more serious. Please do not stop or change blood pressure medication without consulting your neurologist or physician.
-
Anxiety and tremor feed each other. Stress activates the sympathetic nervous system, which in turn worsens tremor, which causes more anxiety. Breaking this cycle often requires addressing both the physical cause (blood pressure) and the psychological contributor (stress and anxiety). If you have tremors, keeping a diary of when they worsen and what triggers them can be extremely helpful information for your doctor.
References
- Pankratz N, et al. "Postural hand tremor and incident hypertension in young to middle-aged adults: the Bogalusa Heart Study." Journal of the Neurological Sciences, 2019.
- Fazekas F, et al. "MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging." American Journal of Neuroradiology, 1987.
- Bhatia KP, et al. "Consensus Statement on the classification of tremors. From the task force on tremor of the International Parkinson and Movement Disorder Society." Movement Disorders, 2018.
- Garber JR, et al. "Clinical Practice Guidelines for Hypothyroidism in Adults." Thyroid, American Thyroid Association, 2012.
- Pengo V, Tripodi A, et al. "Update of the guidelines for lupus anticoagulant detection." Journal of Thrombosis and Haemostasis, 2009.