Clinical Summary
A 58-year-old male commercial airline pilot from the United Kingdom presented with progressive numbness in all four limbs and worsening gait instability. Previously misdiagnosed as Guillain-Barré Syndrome (GBS) and treated with intravenous immunoglobulin (IVIg) in the UK without improvement, the patient sought a second opinion in India. Following a comprehensive neurological evaluation by Dr. Bhupesh Kumar Mansukhani at NeuroMet Wellness Care & Diagnostics, Gurgaon, the diagnosis was corrected to Multiple Sclerosis (MS). He was initiated on Ocrelizumab (Ocrevus), a high-efficacy disease-modifying therapy, and has shown significant functional improvement over eighteen months of follow-up, though a new episode of right optic neuritis is currently under evaluation.
Patient Presentation
The patient, a 58-year-old British national working as a commercial airline pilot, first noticed numbness creeping into both feet and hands over several weeks. As the weeks passed, his balance deteriorated. For a professional pilot, even subtle gait instability is a career-threatening problem that demands immediate attention.
He initially consulted the National Health Service (NHS) in the United Kingdom, where a clinical assessment led to a working diagnosis of Guillain-Barré Syndrome (GBS, an acute condition where the body's immune system attacks the peripheral nerves, often causing ascending weakness). He received a course of IVIg (intravenous immunoglobulin, a treatment that modulates the immune system by infusing concentrated antibodies), the standard first-line therapy for GBS. However, there was no meaningful clinical improvement.
Frustrated by the lack of progress and with persistent symptoms affecting his daily life and career, the patient travelled to India for a fresh evaluation and was referred to Dr. Bhupesh Kumar Mansukhani, Neurologist and Director at NeuroMet Wellness Care & Diagnostics, Gurgaon.
Clinical Examination
On initial examination by Dr. Bhupesh Kumar Mansukhani, the patient was alert and oriented. Key neurological findings included:
- Motor power: Approximately 4/5 on the MRC scale in both upper and lower limbs (meaning mild but definite weakness; the patient could move against resistance, but not at full strength)
- Gait: Unsteady, wide-based gait with difficulty in tandem walking, consistent with a combination of pyramidal and posterior column involvement
- Sensory examination: Diminished sensation to light touch and vibration in a glove-and-stocking distribution across all four limbs
- Deep tendon reflexes: Brisk in both upper and lower limbs. This was a critical distinguishing feature, as GBS typically produces hyporeflexia or areflexia
- Fundoscopy: Normal optic discs bilaterally at initial presentation
- Plantar responses: Equivocal
The presence of brisk reflexes in a patient labelled as GBS was the first major red flag. GBS is a disease of peripheral nerves and characteristically produces absent or diminished reflexes. Brisk reflexes point squarely toward a central nervous system process, and that shifted the diagnostic suspicion toward demyelinating disease of the brain and spinal cord.
Investigations & Findings
MRI Brain with Contrast
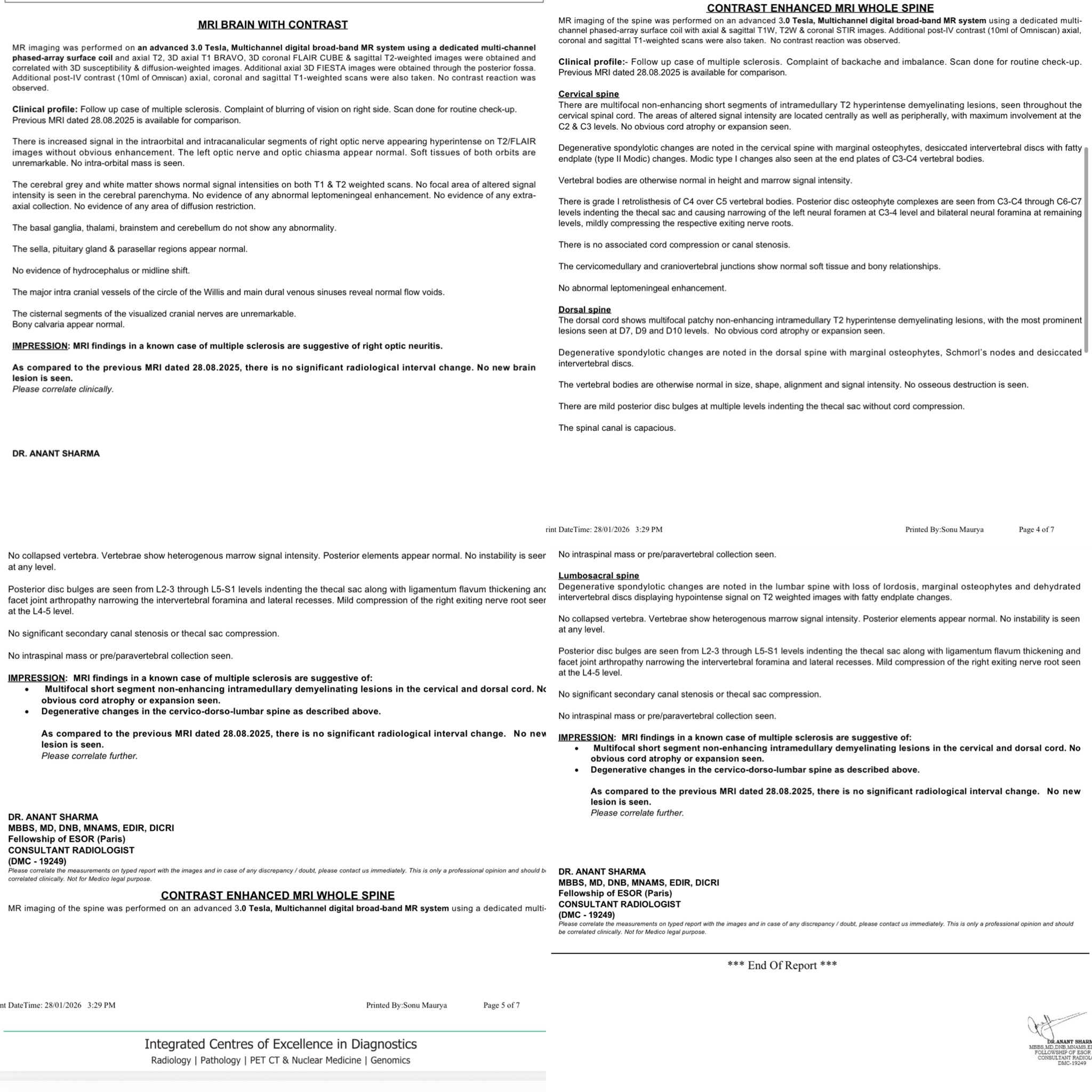
The initial MRI brain (not available for this report) had shown findings consistent with MS. The follow-up MRI brain with contrast (January 2026, approximately 18 months into treatment) revealed:
- Right optic nerve: Increased T2/FLAIR signal in the intraorbital and intracanalicular segments (the portion of the optic nerve within the eye socket and bony canal), suggestive of right optic neuritis (inflammation of the nerve that carries visual information from the eye to the brain). Notably, there was no contrast enhancement, suggesting a subacute or chronic phase.
- Brain parenchyma: Normal grey and white matter signal. No new demyelinating plaques. No diffusion restriction. No leptomeningeal enhancement.
- Comparison with previous MRI (August 2025): No new brain lesions. No significant interval change.
MRI Whole Spine with Contrast (January 2026)
Cervical spine:
Multifocal short-segment, non-enhancing T2 hyperintense intramedullary demyelinating lesions (bright spots within the spinal cord on MRI, indicating areas where the myelin sheath has been damaged) throughout the cervical cord, with maximal involvement at C2 and C3 levels. Lesions were located both centrally and peripherally, a pattern typical of MS. No cord atrophy or expansion was seen. Superimposed degenerative spondylotic changes with disc osteophyte complexes from C3-C4 through C6-C7 and grade I retrolisthesis of C4 over C5 were also noted.
Dorsal (thoracic) spine:
Multifocal patchy non-enhancing intramedullary demyelinating lesions, most prominent at D7, D9, and D10 levels. No cord atrophy or expansion.
Lumbosacral spine:
Multilevel degenerative changes with posterior disc bulges from L2-3 through L5-S1, ligamentum flavum thickening, and facet arthropathy. Mild compression of the right exiting nerve root at L4-5. No intraspinal mass or collection.
Comparison with August 2025 MRI: No new spinal lesions. No significant interval change.
Cerebrospinal Fluid (CSF) Analysis
- Oligoclonal bands (OCBs): Positive (OCBs are bands of immunoglobulins found in the CSF but not in the blood; their presence strongly supports an inflammatory process within the central nervous system and is one of the hallmarks of MS)
- Total protein: Mildly elevated at approximately 120 mg/dL (normal range is typically 15 to 45 mg/dL; mild elevation is common in MS)
- Kappa free light chains: Positive (an emerging biomarker that adds further diagnostic weight toward MS, reflecting intrathecal immunoglobulin production)
Routine Pre-Treatment Workup
Liver function tests (LFT) and kidney function tests (KFT) were within normal limits. Complete blood count and infection screening were satisfactory for initiation of immunosuppressive therapy.
Diagnosis
The final diagnosis was Relapsing-Remitting Multiple Sclerosis (RRMS) based on:
- Clinical: Progressive limb numbness, gait instability, and upper motor neuron signs (brisk reflexes), with dissemination in time evidenced by the new optic neuritis episode
- Radiological: Multifocal demyelinating lesions in the brain (initial MRI), cervical cord, and dorsal cord, demonstrating dissemination in space across at least three CNS regions (periventricular/juxtacortical, spinal cord, optic nerves)
- CSF: Positive OCBs and kappa free light chains, supporting intrathecal inflammation
- Exclusion of mimics: The lack of response to IVIg, brisk reflexes, central cord lesion pattern, and positive OCBs effectively ruled out GBS
The initial misdiagnosis of GBS is an important teaching point. While both conditions can present with limb numbness and weakness, the reflex pattern, CNS imaging findings, and CSF profile are fundamentally different. GBS involves peripheral nerve demyelination with areflexia; MS involves central nervous system demyelination with hyperreflexia.
Treatment Approach
Given the high spinal cord lesion burden, the patient's age, and the need for a therapy with robust efficacy and a manageable safety profile, Dr. Bhupesh Kumar Mansukhani opted for Ocrelizumab (Ocrevus), an anti-CD20 monoclonal antibody that depletes B-lymphocytes, a key driver of the inflammatory cascade in MS.
Dosing protocol (per standard guidelines):
- Initiation cycle: 600 mg administered as two 300 mg intravenous infusions, separated by 14 days
- Maintenance cycles: 600 mg (as two divided doses of 300 mg) every six months
The patient has completed the initiation cycle and two subsequent maintenance infusions to date. All infusions were well tolerated with no significant infusion-related reactions. Standard pre-medication with methylprednisolone, diphenhydramine, and paracetamol was administered before each infusion.
Prior to initiation, the patient had received only IVIg for the incorrect diagnosis of GBS. No prior disease-modifying therapy for MS had been used, making Ocrelizumab his first-line DMT, consistent with the growing "hit hard, hit early" approach in MS management.
Outcome & Follow-Up
At the 18-month mark, the patient has shown significant clinical improvement:
- Walking: Substantially improved from baseline. The patient is ambulatory and independently mobile, a marked change from the unsteady gait at presentation.
- Limb strength: Functionally improved, though formal MRC grading at the most recent visit is pending.
- Radiological stability: The January 2026 MRI of the brain and whole spine shows no new lesions compared to the August 2025 scan. The existing cervical and dorsal cord lesions are stable and non-enhancing, a reassuring sign that the disease is not actively inflammatory.
However, the patient has developed a new complaint of blurring of vision in the right eye. The MRI brain shows T2/FLAIR hyperintensity in the right optic nerve without enhancement, suggestive of right optic neuritis. This is currently being evaluated with visual evoked potentials (VEP), visual acuity and field testing, and optical coherence tomography (OCT) to determine whether this represents a true clinical relapse on Ocrelizumab or a subclinical radiological finding becoming symptomatic.
If confirmed as a breakthrough relapse, this would prompt a reassessment of treatment adequacy, including checking B-cell repopulation kinetics, adjusting infusion intervals, or considering escalation to therapies such as Natalizumab or Cladribine depending on the clinical picture.
Clinical Pearls
- Brisk reflexes in a "GBS" patient should immediately raise suspicion for a central nervous system process. GBS produces peripheral nerve demyelination with hyporeflexia or areflexia, never hyperreflexia. This single clinical finding, if recognized early, could have prevented months of diagnostic delay.
- Kappa free light chains in CSF are an increasingly validated biomarker for MS, with some studies suggesting higher sensitivity than traditional OCBs. When positive alongside OCBs, the diagnostic confidence for intrathecal inflammation is very high.
- Ocrelizumab as first-line high-efficacy DMT is supported by current evidence, particularly in patients with high lesion burden and significant disability at diagnosis. The "hit hard, hit early" paradigm aims to prevent irreversible axonal damage during the window of active inflammation.
- Radiological stability does not guarantee freedom from clinical relapses. New optic neuritis on maintenance Ocrelizumab, as in this case, warrants urgent evaluation including B-cell monitoring and potential treatment adjustment. Not every breakthrough event means treatment failure, but it demands attention.
About the Author
This case was managed by Dr. Bhupesh Kumar Mansukhani, MBBS (Australia), MD (Medicine), DM (Neurology), Fellow in Stroke Medicine and Advanced Neurological Disorders (Harvard Medical School, USA). Neurologist and Director, NeuroMet Wellness Care and Diagnostics, Gurgaon.
For appointments: https://www.neurometwellness.com/booking.php
Tags: Multiple Sclerosis | Ocrelizumab | Optic Neuritis | GBS Misdiagnosis | Neuroimmunology
Patient details have been de-identified and shared with appropriate consent. This case study is for educational purposes only.