Tags: Stroke | Atypical Presentation | Multifocal Infarct | Small Vessel Disease | Protein S Deficiency | Outpatient Stroke Management Category: NeuroMet Case Studies
Clinical Summary
Most people picture a stroke as sudden paralysis — a face drooping, an arm that won't lift, speech that disappears in an instant. But stroke doesn't always announce itself that loudly. In this case, a 57-year-old woman walked into the clinic with a headache, a fleeting episode of slurred speech, and something she could only describe as "brain fog." There was no arm weakness. No obvious facial asymmetry. Just subtle, easy-to-dismiss symptoms sitting on top of a blood pressure of 180/95 mmHg and a blood sugar of 345 mg/dL. An MRI confirmed what the examination hinted at — a multifocal acute ischemic stroke involving three separate brain regions. What followed was a deep diagnostic workup, a difficult conversation about admission, and a decision to manage one of neurology's most serious emergencies entirely in an outpatient setting — because sometimes, that is the only option available.
Patient Presentation
A 57-year-old woman presented to the neurology OPD with a 3-day history of persistent right-sided, dull, unilateral headache. Two days prior to her visit, she had experienced a transient episode of dysarthria (slurring of speech that lasted briefly and then resolved on its own). She also complained of episodes of cognitive fogginess — difficulty concentrating, an unusual sense of mental sluggishness, and what she described as "irrelevant thoughts coming and going." Additionally, she reported diplopia (double vision) and mild blurring of vision.
Crucially, there were no focal motor deficits — her arms and legs moved normally, her face was symmetric, and she had no obvious limb weakness. This absence of classical motor signs made the clinical picture deceptively subtle and significantly complicated early recognition.
Her past medical history was notable for hypertension, though her degree of control was unclear at presentation. There was no prior documented diabetes, no prior stroke or TIA history, and no known cardiac disease.
Clinical Examination
Vitals at Presentation:
| Parameter | Value |
|---|---|
| Blood Pressure | 180/95 mmHg — severely elevated |
| Random Blood Sugar (RBS) | 345 mg/dL — severely elevated |
Neurological Examination:
Cranial nerve assessment revealed subtle signs consistent with posterior circulation involvement — mild visual disturbance and subjective diplopia without overt cranial nerve palsy. Limb power was preserved bilaterally (5/5 in all four limbs). Sensory examination, coordination, and gait were grossly intact.
The combination of a severely elevated blood pressure, acute hyperglycemia, and posterior circulation symptoms in the absence of obvious motor deficits raised immediate clinical concern for an ongoing cerebrovascular event.
Investigations & Findings
Neuroimaging
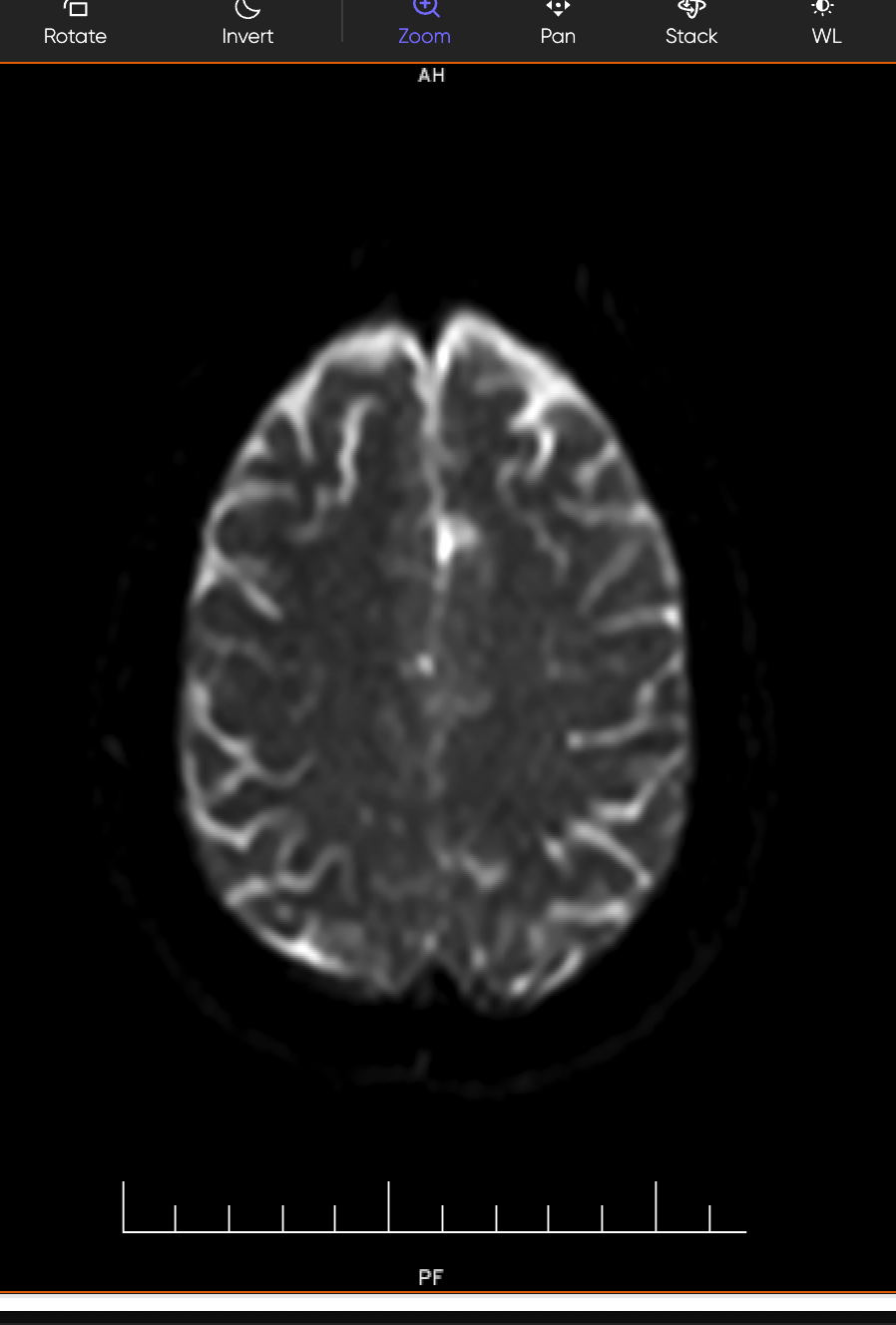
MRI Brain (DWI/ADC — Diffusion Weighted Imaging):
This is the gold-standard sequence for detecting acute stroke — it lights up areas of fresh brain injury within minutes of onset. The MRI confirmed multifocal acute ischemic infarcts in three separate regions:
- Left Corona Radiata — a deep white matter structure involved in motor and cognitive relay pathways
- Right Temporo-Occipital White Matter — associated with visual processing and sensory integration
- Right Occipital Lobe — the brain's primary visual cortex, explaining the patient's visual symptoms
The report also noted "mild chronic ischemic microvascular changes" — evidence that the brain's small vessels had been silently suffering damage for some time, even before this acute event.
CT Angiography (Brain + Neck Vessels):
No large vessel occlusion (LVO) or significant stenosis was identified. Atherosclerotic calcific and soft plaques were noted along the arch of the aorta, but without any significant luminal narrowing. This ruled out a major arterial blockage as the culprit.
Thrombophilia & Coagulation Screen
| Test | Result | Reference Range | Interpretation |
|---|---|---|---|
| PT/INR | 1.06 | 0.9–1.1 | Normal |
| APTT | 27.2 sec | 26.9–36.4 sec | Normal |
| Protein C Activity | 118% | 70–130% | Normal |
| Protein S Activity | 18.1% | 60–140% | ⚠️ Significantly Low |
| Anti-Thrombin III | 105% | 80–120% | Normal |
| Lupus Anticoagulant | Absent | Absent | Normal |
Protein S is a naturally occurring anticoagulant — one of the body's own blood-thinning proteins. A deficiency significantly increases the risk of abnormal clot formation inside blood vessels (thrombosis), and is a recognised cause of stroke, particularly in multifocal presentations.
Echocardiogram (2D Echo)
No cardioembolic source was found — no clots, vegetation, or pericardial effusion. However, the heart revealed clear signs of chronic hypertensive strain:
- Concentric Left Ventricular Hypertrophy (LVH): Septal and posterior wall thickness of 12 mm — the heart muscle had thickened over years of working against uncontrolled high blood pressure
- Type 1 LV Diastolic Dysfunction: Stiff, non-compliant ventricle — a precursor to further cardiac complications
- LVEF = 60%: Preserved ejection fraction — the heart was still pumping effectively despite the structural changes
Comprehensive Bloodwork
| Parameter | Result | Reference | Significance |
|---|---|---|---|
| HbA1c | 13.1% | < 5.7% | Severe, newly diagnosed uncontrolled diabetes |
| RBS (presentation) | 345 mg/dL | 70–140 mg/dL | Acute severe hyperglycemia |
| C-Reactive Protein (CRP) | Elevated | Normal | Active systemic inflammation |
| Free T3 | 2.14 pg/mL | 2.42–4.36 | Low — possible sick euthyroid / subclinical thyroid dysfunction |
| Free T4 | 1.72 ng/dL | 0.95–1.57 | Slightly elevated |
| TSH | 3.0 µIU/mL | 0.27–4.20 | Normal |
| Alkaline Phosphatase | 133 U/L | 35–104 | Mildly elevated |
| Inorganic Phosphorus | 4.81 mg/dL | 2.5–4.5 | Slightly elevated |
The HbA1c of 13.1% — a measure of average blood sugar over the preceding 3 months — was one of the most striking findings. This confirmed severe, longstanding, previously undiagnosed diabetes, a condition known to directly damage the walls of small blood vessels throughout the body, including those supplying the brain.
Diagnosis
Acute Multifocal Ischemic Stroke — Small Vessel Disease Pattern
Etiology: Multifactorial — Hypertensive Small Vessel Disease + Severe Uncontrolled Diabetes + Protein S Deficiency + Systemic Inflammation
Differentials Considered and Addressed:
- Large Vessel Atherosclerosis: Ruled out — CT Angiography showed no significant stenosis or LVO
- Cardioembolic Stroke: Ruled out — 2D Echo showed no thrombus, vegetation, or significant structural source
- Autoimmune / Vasculitic Stroke: Clinically low probability given the metabolic context; Lupus Anticoagulant negative
- RCVS / Vasospasm: Less likely given the chronic microvascular background changes and multifocal distribution
Pathophysiological Synthesis — The "Perfect Storm":
This patient's multifocal infarcts were the end result of several converging pathological forces:
- Severe, uncontrolled diabetes (HbA1c 13.1%) — causing direct microvascular endothelial injury and a pro-inflammatory, pro-thrombotic state
- Severe, longstanding hypertension (BP 180/95) — driving small vessel wall hyalinisation and accelerating cerebral microangiopathy, as evidenced by LVH on echo
- Protein S deficiency (18.1%) — impairing the natural anticoagulant cascade, amplifying the thrombotic tendency
- Elevated CRP — reflecting systemic vascular inflammation compounding the risk
No single factor explained the stroke on its own. Together, they created conditions in which small cerebral vessels could not be protected, and multiple small infarcts occurred simultaneously across different brain territories.
Treatment Approach
The Difficult Conversation
Standard-of-care guidelines strongly recommend immediate inpatient admission for confirmed acute ischemic stroke — for continuous monitoring, IV access, stroke unit nursing, and early rehabilitation. This recommendation was clearly communicated to the patient and her family.
The patient declined admission, citing financial constraints and lack of health insurance. After detailed counseling regarding the risks of outpatient management — including the possibility of early neurological deterioration, recurrent stroke, and the importance of compliance — informed consent was obtained, and a carefully structured outpatient management protocol was initiated.
This decision reflects the reality of neurology practice in resource-limited settings: the textbook ideal must sometimes be adapted, with clear documentation, robust counseling, and a rigorous follow-up framework.
Outpatient Management Protocol
1. Antiplatelet Therapy (Dual)
- Aspirin 150 mg (Ecosprin) + Clopidogrel 75 mg (Plavix) — dual antiplatelet therapy to reduce recurrent stroke risk during the highest-risk early period
2. High-Intensity Statin
- Atorvastatin 40 mg (Storvas) — for vascular stabilisation, plaque regression, and anti-inflammatory effects
3. Antihypertensive Therapy
- Telmisartan + Amlodipine combination — targeting aggressive BP reduction given hypertensive small vessel disease as a primary driver
4. Diabetes Management
- Metformin + Vildagliptin initiated — patient declined insulin despite HbA1c of 13.1%
- Referral to endocrinologist for optimisation and insulin initiation plan
5. Patient Engagement & Self-Monitoring
- Strict home BP and blood sugar charting — twice-daily monitoring with a diary
- Detailed written instructions on warning signs requiring emergency attendance
- Family education on stroke recognition and response
Outcome & Follow-Up
At one-month follow-up, the patient returned to the OPD clinically stable, with no new neurological events reported.
| Parameter | At Presentation | At 1-Month Follow-Up |
|---|---|---|
| Blood Pressure | 180/95 mmHg | 148/83 mmHg |
| Neurological Status | Active acute infarcts | Stable — no new events |
| Adherence | — | Good — continued OPD plan |
The reduction in blood pressure from 180/95 to 148/83 mmHg represented a meaningful early win, significantly reducing the haemodynamic stress on already-vulnerable cerebral small vessels. Ongoing referral to endocrinology was maintained, and the follow-up schedule continued with close neurological surveillance.
Clinical Pearls / Teaching Points
-
Stroke can wear a mask. When headache, brain fog, diplopia, and transient speech slurring coexist with a BP of 180/95 mmHg — that is a neurological emergency until proven otherwise, regardless of preserved limb power. Posterior circulation strokes are classically under-recognised because motor deficits are often absent.
-
Metabolic disease is not a background risk — it is an active driver. An HbA1c of 13.1% represents months of uncontrolled glucose bathing the vessel walls in inflammatory mediators. Uncontrolled diabetes and hypertension together create a cerebrovascular environment primed for small vessel disease and multifocal infarction.
-
Always complete the thrombophilia screen in multifocal stroke. This case would have been incomplete without the Protein S level. A deficiency of 18.1% — a natural anticoagulant — was a key piece of the etiological puzzle and has direct implications for long-term anticoagulation decisions.
-
Outpatient stroke management is possible — but demands precision. With informed consent, detailed counseling, structured pharmacotherapy, and a robust monitoring plan, selected patients who cannot access inpatient care can be safely managed in an OPD setting. The clinician's responsibility is to document, educate, and follow up relentlessly.
This case was managed by Dr. Bhupesh Kumar Mansukhani, MBBS (Australia), MD (Medicine), DM (Neurology), Fellow in Stroke Medicine and in Advance Neurological Disorders (Harvard Medical School, USA) — Neurologist & Director, NeuroMet Wellness Care and Diagnostics, Gurgaon. For appointments: www.neurometwellness.com | Personal Website: www.drbhupesh.com
Patient details have been de-identified and shared with appropriate consent. This case study is for educational purposes only.
References
- Powers WJ et al. — 2019 AHA/ASA Guidelines for the Early Management of Acute Ischemic Stroke. Stroke. 2019;50(12):e344–e418.
- Dyken ME, Biller J. — Protein S Deficiency and Ischemic Stroke: A Systematic Review. Cerebrovasc Dis. 2003.
- Tuttolomondo A et al. — Diabetes Mellitus as a Risk Factor for Cerebrovascular Disease. Curr Pharm Des. 2012;18(35):5606–5622.
- Vermeer SE et al. — Incidental Findings on Brain MRI in the General Population. N Engl J Med. 2007;356(18):1821–1828. (White matter changes and cerebral small vessel disease)
- Banerjee C, Chimowitz MI. — Stroke Caused by Atherosclerosis of the Major Intracranial Arteries. Circ Res. 2017;120(3):502–513.
- Boehme AK, Esenwa C, Elkind MSV. — Stroke Risk Factors, Genetics, and Prevention. Circ Res. 2017;120(3):472–495.