Tags: Stroke | Young Stroke | Thrombolysis | Cannabis & Stroke | Lifestyle Neurology Category: NeuroMet Case Studies
Clinical Summary
A 36-year-old man walked into the emergency room with a drooping face, slurred speech, and weakness on one side of his body — the classic red flags of a stroke. What followed was a race against time: a successful thrombolysis within 45 minutes. But the more revealing story unfolded during the workup that came after, when every conventional cause came back negative — and the real culprit turned out to be a decades-long history of smoking, cannabis use, and a recent binge on alcohol. This case is a reminder that stroke does not discriminate by age, and that lifestyle choices carry neurological consequences that can arrive suddenly and without warning.
Patient Presentation
A 36-year-old male was brought to the emergency room by his family with a sudden onset of left-sided weakness (loss of power in the left arm and leg), dysarthria (slurred, difficult-to-understand speech), and left-sided facial deviation (drooping of the face on one side). The symptoms had begun acutely, with no preceding headache or loss of consciousness.
On arrival, the patient's NIHSS score (NIH Stroke Scale — a standardized tool used to measure stroke severity, scored 0–42) was 7, placing him in the moderate stroke category.
His past medical history was unremarkable for hypertension, diabetes, or heart disease — all the usual suspects in a stroke presentation. He had no prior history of neurological events. What was relevant, however, emerged gradually during history-taking: 17 years of active cigarette smoking, habitual use of marijuana, hash, and cannabis, and a history of recent heavy alcohol consumption.
Clinical Examination
Neurological Examination:
| Limb | Power (MRC Scale) |
|---|---|
| Right Upper Limb | 5/5 (Normal) |
| Right Lower Limb | 5/5 (Normal) |
| Left Upper Limb | 3/5 (Significant weakness) |
| Left Lower Limb | 3/5 (Significant weakness) |
Facial examination confirmed left-sided lower motor neuron-pattern facial deviation. Speech was dysarthric but the patient remained conscious and oriented. Cranial nerve examination, coordination, and sensory testing were consistent with a right-sided deep hemispheric insult.
Investigations & Findings
Neuroimaging
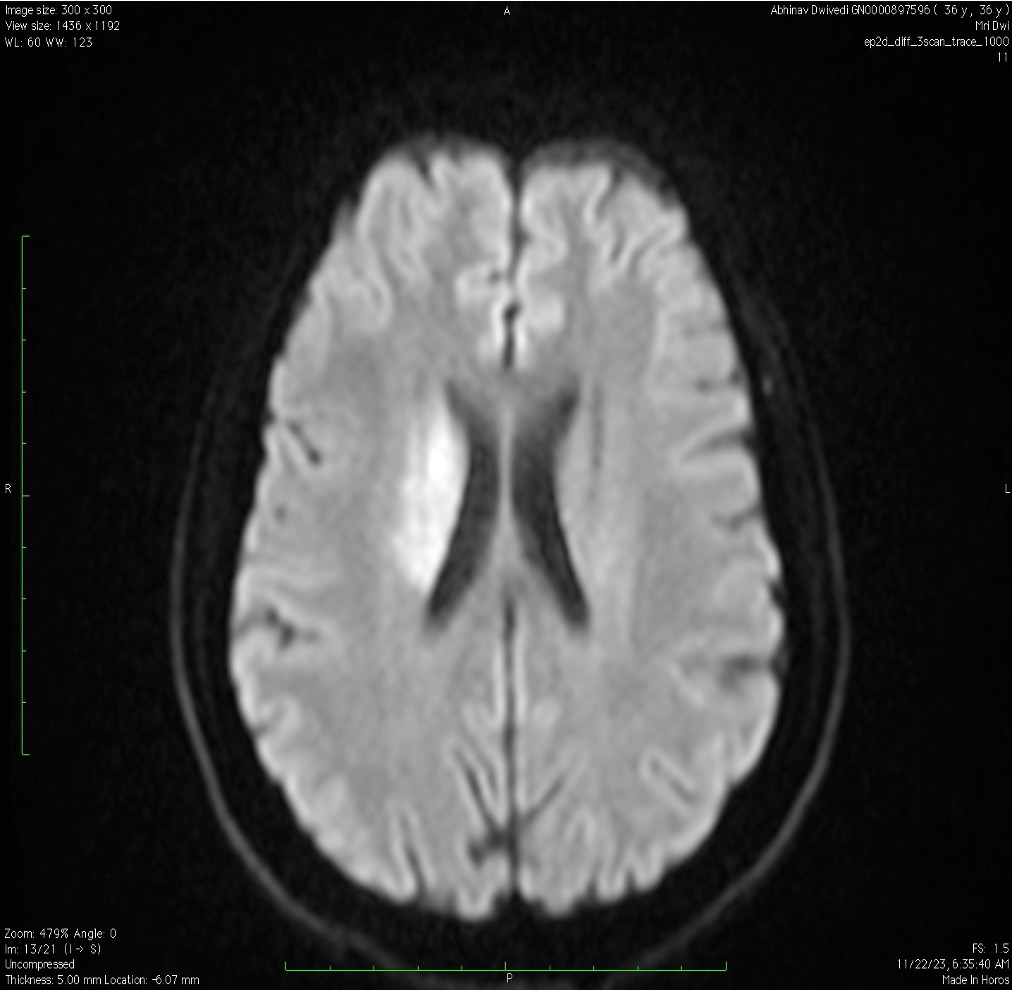
MRI Brain (DWI/ADC sequences):
Diffusion-weighted imaging — which highlights areas of fresh brain injury with high sensitivity — confirmed an acute infarct in the right Globus Pallidus and right Putamen (a region in the deep part of the brain called the basal ganglia, responsible for movement coordination and motor control).
CT Angiography (Brain + Neck Vessels):
No LVO (Large Vessel Occlusion — a blockage in one of the major arteries supplying the brain) was identified. The major cerebral and neck vessels appeared patent.
NCCT Head (Non-Contrast CT) at 12 hours post-thrombolysis:
No hemorrhagic transformation. The thrombolysis was safe and successful.
Young Stroke Workup (All Negative)
An extensive workup for less common causes of stroke in a young individual was sent, and all returned negative:
- Autoimmune / Vasculitic Screen: ANA, ANCA, APLA (Antiphospholipid Antibodies), ACE — all negative
- Infective: VDRL (syphilis screen) — negative
- Cardiac Workup: 2D Echocardiography, Transesophageal Echocardiography (TEE), 72-hour Holter monitoring — no cardioembolic source identified
With conventional causes ruled out, attention turned firmly toward lifestyle and substance use.
Diagnosis
Acute Ischemic Stroke — Right Basal Ganglia (Right Globus Pallidus + Putamen)
Etiology: Lifestyle-Linked / Substance-Associated Ischemia
The final etiological classification was cryptogenic stroke with strong association to substance use, in line with published literature linking cannabis and tobacco use to early-onset ischemic cerebrovascular events.
Differentials Considered and Ruled Out:
- Cardioembolic stroke (ruled out: negative TEE, Holter, Echo)
- Vasculitic/autoimmune stroke (ruled out: negative ANA, ANCA, APLA, ACE)
- Infectious etiology (ruled out: VDRL negative)
- Large vessel atherosclerosis (ruled out: CTA showing no LVO or significant stenosis)
Pathophysiological Insight:
Cannabis exerts its cerebrovascular effects through multiple mechanisms. As documented in literature (Asif B. et al.), marijuana use is linked with:
- Elevated carboxyhemoglobin levels (carbon monoxide displacing oxygen from red blood cells, reducing oxygen delivery to brain tissue)
- Orthostatic hypotension (drop in blood pressure on standing, reducing cerebral perfusion)
- Tachycardia (increased heart rate, altering cardiac output and cerebral hemodynamics)
Combined with chronic tobacco-induced endothelial injury and the pro-thrombotic milieu of recent binge alcohol intake, the stage was set for a deep cerebral infarct in a young man whose vessels were aging far faster than his years.
Treatment Approach
Acute Management: Thrombolysis
Given the confirmed ischemic nature on imaging, absence of contraindications, and a presentation within the thrombolysis window, the decision was made to administer IV Alteplase (rTPA) at 0.9 mg/kg.
- 10% of the dose administered as an IV bolus
- Remaining 90% infused over one hour
- Door-to-Needle Time: 45 minutes (the time from the patient entering the hospital to receiving the clot-busting drug — international guidelines recommend under 60 minutes)
The patient was monitored in the ICU post-thrombolysis. A follow-up CT scan at 12 hours confirmed no bleeding — a key safety milestone.
Secondary Prevention
Following stabilization, the treatment plan included:
- Dual Antiplatelet Therapy (DAPT): Aspirin + Clopidogrel to reduce recurrence risk
- High-Intensity Statin: For vascular stabilization and lipid management
- Neurological Monitoring: Continuous observation for any deterioration
- Neuro-Rehabilitation: Early physiotherapy and speech therapy initiated to maximize functional recovery
Outcome & Follow-Up
The patient showed gradual improvement in left-sided power following thrombolysis. Neurorehabilitation was initiated early, which is critical for functional recovery following basal ganglia infarcts. At discharge, the patient was ambulatory with mild residual weakness, and speech had significantly improved.
Discharge Counseling included:
- Structured de-addiction support for cannabis, hash, and tobacco
- Smoking cessation counseling with pharmacotherapy options discussed
- Strict avoidance of alcohol, particularly binge episodes
- Regular outpatient follow-up with neurology for surveillance and stroke prevention
The patient and his family were counseled extensively that a recurrent stroke, in the absence of lifestyle modification, carries an even higher risk of permanent disability.
Clinical Pearls / Teaching Points
-
Stroke does not spare the young. Any acute focal neurological deficit in a young adult must be treated as a stroke until proven otherwise — age is not a protective factor when lifestyle risk is high.
-
A negative conventional workup is not the end of the story. When autoimmune, cardiac, and large-vessel causes are ruled out, a detailed substance and lifestyle history becomes the most important diagnostic tool in the room.
-
Cannabis is not benign. Its cerebrovascular effects — carboxyhemoglobin elevation, postural hypotension, tachycardia — are well-documented and clinically meaningful. Routine substance screening should be considered in all young stroke cases.
-
Time is brain — and 45 minutes matters. A door-to-needle time of 45 minutes in a young stroke without LVO demonstrates that thrombolysis remains a powerful intervention even in atypical presentations, provided eligibility criteria are carefully met.
This case was managed by Dr. Bhupesh Kumar Mansukhani, MBBS (Australia), MD (Medicine), DM (Neurology), Fellow in Stroke Medicine and in Advance Neurological Disorders (Harvard Medical School, USA) — Neurologist & Director, NeuroMet Wellness Care and Diagnostics, Gurgaon. For appointments: www.neurometwellness.com | Personal Website: www.drbhupesh.com
Patient details have been de-identified and shared with appropriate consent. This case study is for educational purposes only.
References
- Asif B et al. — Cannabis and Stroke: Mechanisms, Evidence, and Clinical Implications. J Stroke Cerebrovasc Dis. [PMID-linked literature on cannabis-associated cerebrovascular events]
- Powers WJ et al. — 2019 AHA/ASA Guidelines for the Early Management of Acute Ischemic Stroke. Stroke. 2019;50(12):e344–e418.
- Singhal AB et al. — Reversible Cerebral Vasoconstriction Syndromes and Substance Use. Ann Neurol. 2005.
- Hackam DG. — Cannabis and Stroke: Systematic Appraisal of Case Reports. Stroke. 2015;46(3):852–856.
- Wolff V, Jouanjus E. — Strokes are possible complications of cannabinoids use. Epilepsy Behav. 2017;70:355–363.