Doctors have a nickname for it. It is not a kind one.
They call it the suicide headache.
Not because it is dramatic, but because patients have described the pain as worse than childbirth, worse than a kidney stone, worse than a fracture. People do not lie still through it. They pace. They rock. They press their fists into their eye socket. Some hit their head against the wall, not in panic, but because the competing pain is the only thing that distracts from it.
And here is the cruel part. This condition, one of the most severe pains in all of medicine, is one of the most commonly misdiagnosed. Patients spend years being told it is sinusitis. Or a dental problem. Or "just a bad migraine." They visit ENT surgeons, dentists, and three different doctors before anyone says the actual words: cluster headache.
If you, or someone you love, have a brutal one-sided headache that arrives like clockwork, this post is for you.
What is cluster headache, actually?
Cluster headache belongs to a family of conditions neurologists call the trigeminal autonomic cephalalgias. That is a mouthful, so let us unpack it, because the name is the diagnosis.
Trigeminal refers to the trigeminal nerve, the main sensory nerve of the face. Autonomic refers to the automatic nervous system that controls things like tears, nasal congestion, and pupil size. Cephalalgia simply means head pain.
Put together: this is a headache that fires through the facial nerve system and drags the body's automatic plumbing along with it. That combination, severe one-sided pain plus automatic signs on the same side, is the fingerprint of the disease. Nothing else looks quite like it.
It is rare, affecting roughly one in a thousand people. But because it is so often mislabelled, the real number of people suffering quietly is almost certainly higher.
The fingerprint: how to recognise it
Cluster headache is one of the few headaches that can be diagnosed almost entirely on the story. The pattern is that distinct.
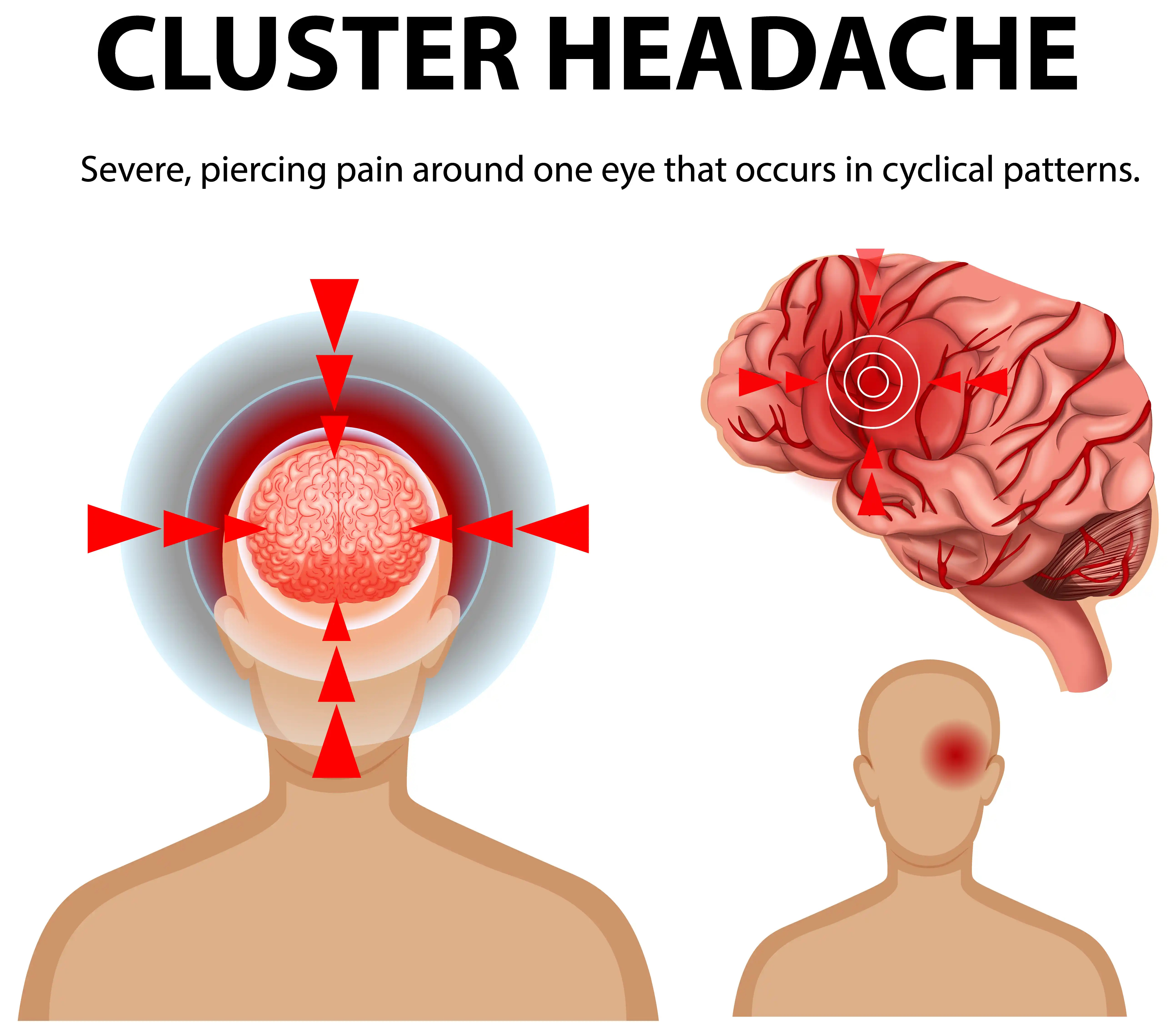
The pain is strictly one-sided. Always the same side during a bout, almost always centred around or behind one eye, sometimes spreading to the temple or jaw. It does not wander to the other side mid-attack.
It is severe and sharp, not a dull ache. Patients describe it as a hot poker, a drill, a knife behind the eye. This is not the band-around-the-head pressure of a tension headache.
It comes with autonomic signs on the same side. This is the giveaway. On the painful side you may see a red, watering eye; a blocked or running nostril; a drooping or swollen eyelid; a smaller pupil; sweating on that side of the face. One eye crying, one nostril blocked, all on the side that hurts.
Patients are restless. This is the single best clue that separates it from migraine. A migraine sufferer wants to lie still in a dark room. A cluster patient cannot keep still. They pace, they rock, they cannot sit through the pain.
The attacks are short but vicious. Each one typically lasts between fifteen minutes and three hours, then switches off, often as suddenly as it began.
Why it is called "cluster": the clock inside the disease
The name comes from the way the attacks group together in time, and this rhythm is genuinely strange.
Attacks come in bouts, periods of weeks to months where they strike daily, sometimes several times a day, up to eight in twenty four hours. Then the bout ends and the person may be completely pain-free for months or even years before the next one.
Stranger still, the attacks often keep a schedule. Many patients are woken at the same hour every night, frequently in the early hours, almost as if an alarm clock is wired into the disease. Bouts also tend to cluster around the changing of seasons. This circadian and seasonal timing points the finger at the hypothalamus, the brain's master clock, which is now understood to play a central role.
Two main forms exist. In episodic cluster headache, bouts are separated by long pain-free remissions. In chronic cluster headache, the attacks continue with little or no break for a year or more. The chronic form is harder to treat and absolutely needs specialist care.
Who gets it, and what sets it off
Cluster headache tends to begin between the ages of twenty and forty. Historically it was considered far more common in men, though it is increasingly recognised in women too. Smoking is strongly associated with it, and a family history can raise the risk.
During an active bout, certain triggers can reliably set off an attack:
- Alcohol. Even a small amount can provoke an attack within an hour, but only while a bout is running. Between bouts the same drink does nothing. This on-off relationship is itself a diagnostic clue.
- Sleep. Attacks frequently strike during sleep, particularly the first deep sleep cycle of the night.
- Strong smells, heat, and altitude can trigger attacks in some people. Outside of a bout, these triggers usually have no effect, which is part of what makes the condition so confusing to patients.
Cluster headache vs migraine: not the same animal
People lump them together. They should not. The treatment is different, the urgency is different, the experience is different.
A migraine sufferer wants stillness, darkness, and silence. A cluster sufferer cannot stay still. Migraine pain builds and throbs over hours and is often accompanied by nausea and aura. Cluster pain is a sudden, boring, one-sided assault around the eye with watering and congestion, peaking fast and ending fast. Migraine attacks are usually less frequent; cluster attacks can come several times in a single day. The autonomic signs (red watering eye, blocked nostril, drooping lid on one side) are the hallmark of cluster and are not the central feature of typical migraine.
Getting this distinction right is not academic. The wrong label means years of the wrong treatment.
Why it gets missed for years
The eye waters. The nose blocks. The pain sits over the cheek and brow. So patients are told it is sinusitis and handed antibiotics and decongestants that do nothing. The pain centres near the upper teeth, so some end up having dental work for a problem that was never in the tooth. And because it is "just a headache," many do not push for a specialist opinion at all.
The tragedy is that cluster headache is highly treatable once correctly identified. The years of suffering are almost always a diagnostic failure, not a treatment failure.
How a neurologist diagnoses and treats it
Diagnosis is mostly clinical. The pattern is so characteristic that a careful history usually makes the call. A brain MRI is typically done to rule out the rare secondary causes that can mimic it, but the diagnosis itself rests on the story and examination.
Treatment runs on three tracks at once.
Stopping an attack fast (acute treatment). Ordinary painkillers are useless here; the attack is too fast and too severe. The two treatments that genuinely work are high-flow oxygen delivered through a mask, which can abort an attack within minutes, and fast-acting triptan medication given by injection or nasal spray rather than tablet. Speed of delivery is everything.
Bridging through a bout (transitional treatment). To get control quickly while preventive medication builds up, neurologists may use a short course of corticosteroids, or a nerve block such as a greater occipital nerve block. In selected cases, a sphenopalatine ganglion (SPG) block, a quick non-invasive intranasal procedure, can be used to settle the autonomic storm.
Preventing the attacks (preventive treatment). The cornerstone preventive drug is verapamil, a medication that reduces how often attacks occur, used under cardiac monitoring. Other agents are added depending on the case. Newer options, including a specific injectable preventive (a CGRP-targeting antibody) and non-invasive vagus nerve stimulation, have expanded what is possible for difficult cases.
The point is this: cluster headache has real, effective, specific treatments. Suffering through it silently is not the only option, and it is not the right one.
When should you see a specialist in Gurgaon?
You should see a neurologist promptly if you have:
- A severe, strictly one-sided headache around or behind one eye.
- A watering eye, a blocked or running nostril, or a drooping eyelid on the same side as the pain.
- Attacks that come and go in bouts or strike at the same time each day or night.
- Headaches that make you restless and unable to sit still.
- Pain that has been labelled sinus or dental but never truly resolves. This is not a headache to ride out with over-the-counter tablets. It is a specific neurological condition with specific treatments, and the sooner it is correctly named, the sooner the pain stops controlling your life.
Consult a neurologist in Gurgaon
If you recognise this pattern in yourself or someone close to you, a proper evaluation can end years of being misdiagnosed.
NeuroMet Wellness Care and Diagnostics LG-02, Ansals Boom Plaza, Sushant Lok Phase 3, Sector 57, Gurugram, Haryana 122003 +91 88609 22792
Authored by: Dr. Bhupesh Kumar Mansukhani | MBBS (Australia), MD (Medicine), DM (Neurology), Fellow in Stroke Medicine and Advanced Neurological Disorders (Harvard Medical School, USA) Director, NeuroMet Wellness Care and Diagnostics, Gurgaon www.drbhupesh.com
This article is for general educational purposes and is not a substitute for individual medical advice. If you are experiencing a severe or sudden headache, seek medical attention immediately.